Mediation and Moderation of Sleep in Arthritis Fatigue Assignment Sample
INTRODUCTION
Background and Significance
Fatigue and Arthritis. The definition of fatigue is "loss of energy and difficulty to keep a regular schedule"
(Cella et al., 2010). Chronic tiredness is thought to be aberrant and pervasive, occurring in individuals who often do not benefit from standard restorative treatments, in contrast to acute weariness, which is typically tied to a particular cause and is frequently cured by rest (Christodoulou et al., 2014). In older adults, fatigue is a worrying symptom since it is linked to functional impairments and predicts 10-year mortality (Hardy & Studenski, 2008a) (Hardy & Studenski, 2008b).
The impact of arthritis on public health is also significant. In the US, the prevalence of arthritis is 23%, or 54.4 million people, making it the most common kind of adult disease (Sandoval-Rosario et al., 2018). For older persons, arthritis is the main source of impairment (Barbour et al., 2017). Co-morbid conditions including heart disease, obesity, and diabetes place a heavy load on arthritis patients (Havens et al., 2017).
A musculoskeletal disorder called arthritis affects the connective tissues around the joints, including the muscles, tendons, and ligaments (Hootman et al., 2012). Two kinds of arthritis that are of particular importance are rheumatoid arthritis and osteoarthritis. The most prevalent form of arthritis, osteoarthritis (OA), affects over 30 million persons worldwide (CDC, 2020). OA is a chronic degenerative illness and a typical age-related ailment (Anderson & Loeser, 2010). Obesity, physical inactivity, and joint injury are risk factors for OA (Hawker, 2019).
Over 1.3 million persons in the US suffer with rheumatoid arthritis (RA), the second most frequent kind of arthritis (Ma et al., 2014). Although the exact origin of RA is unknown, environmental and genetic factors are considered to be involved (Deane et al., 2017). One of the most costly medical illnesses to treat in US hospitals, RA costs $19.3 billion annually (Birnbaum et al., 2010).
Due to its high prevalence (affecting up to 70% of arthritis patients) and interference with patients' ability to participate in everyday activities, arthritis-related tiredness is a serious problem (Gron et al., 2014; Kirwan et al., 2007; Overman et al., 2016). The biggest indicator of future decreased activity is arthritis fatigue (Murphy et al., 2013).
Reduced exercise for arthritis patients worsens their symptoms as well as any other co-morbidities they may have. In the therapeutic setting, where physical exercise is proven to be beneficial in lowering tiredness symptoms and controlling co-morbidities, arthritis fatigue has an adverse effect on patients by restricting physical activity. (2012) Hotman et al.
There are many variables to consider while assessing the covariates of arthritis tiredness (Hackney et al., 2019) for nursing dissertation. In patients with arthritic fatigue, associations between the modifiable factors of physical activity and sleep have been found (Matura et al., 2018). In addition to behavioural variables, heart disease, obesity, and diabetes co-morbidities may be managed by increasing physical activity and improving sleep quality (Hootman et al., 2012). Thus, the emphasis of this study is on the particular factors of physical activity and sleep and how they relate to arthritis weariness.
Physical Activity, Fatigue, And Sleep. Exercise has been demonstrated to lessen arthritis patients' sensations of weariness (Durcan et al., 2014; Katz et al., 2018; Rongen-van Dartel et al., 2016). Additionally, exercise has been linked to better sleep and arthritis sufferers (Durcan et. al, 2014). Numerous research have shown that physical activity, sleep, and weariness are correlated. Poor sleep is quite common and is closely related to tiredness in older adults with OA (Hardy & Studenski, 2008a). Fatigue and inadequate sleep are associated (Austad et al., 2017). RA fatigue is strongly impacted by physical function and sleep quality (Rongen- van Dartel et al., 2016). Poor sleep, depression, and obesity have all been demonstrated to have a role in the indirect relationship between physical inactivity and tiredness (Katz et al., 2016). Cross-sectional study designs are often used in studies examining the connections between weariness, physical activity, and sleep (Loppenthin, Esbensen, Ostergaard, et al., 2015; Puyraimond-Zemmour et al., 2017; Westhovens et al., 2014).
Although cross sectional designs provide insight into a variety of factors, it may be challenging to establish their causal relationships (Nikolaus et al., 2013; Solem, 2015). Although sleep and physical activity are thought to be variables in arthritic tiredness, the part that sleep plays in this association is unclear (McKenna et al., 2017; Nikolaus et al., 2013). The processes underlying the relationships between the factors of weariness, physical activity, and sleep will be better understood via further study employing randomised controlled trials or longitudinal designs. This study broadens our understanding of the interplay between arthritic fatigue, physical activity, and sleep in a longitudinal setting. This study also emphasises the value of second-generation research to enhance therapeutic tiredness therapies.
Second-generation research. Sleep and physical exercise have been shown to be related to arthritic weariness. Understanding sleep's involvement as a third component in the connection is the next step in increasing our understanding in this area. The importance and function of first- and second-generation research were discussed by Guralnick (1993) in the context of his work on early intervention for children. These categories provide valuable insight into the relevance of third variable research and are pertinent to nursing research (Guralnick, 1993).
In first-generation research, the direct link between variables is shown, and the major influence of one variable on another is examined (Hopwood, 2007). In the first generation of study, the link between the independent and dependent variables is the main emphasis (MacKinnon & Luecken, 2008). Direct impact research does not, however, suit everyone, particularly when it comes to how it may be used in a therapeutic situation. There is now mounting research that suggests a connection exists between arthritic weariness, physical activity, and sleep.
The use of first-generation research led to the conception of second-generation research (Guralnick, 1993). Clinical research must demonstrate more than the presence of an effect (Kraemer et al., 2002), and it is crucial to comprehend how such effects function and their boundary conditions. In second-generation research, the features that combine to best cure a certain ailment under specific circumstances are specified (Hayes & Rockwood, 2017).
Second-Generation Research. Looks at the circumstances in which the major effect(s) between two variables operate. Third (3rd) variable study design serves as a representation of this (Hopwood, 2007). In order to provide physicians insight into current therapies and help them be more effective at providing individualized care, it is crucial to examine the function, importance, and consequences of third factors (Kraemer et al., 2002). Through the use of mediation and moderation techniques, this study investigates the contribution of the third variable impact of sleep onto arthritis tiredness.
Mediation and Moderation Methodology
A conceptual and statistical framework for third (3rd) variable designs that include variables (or groups of variables) that affect the relationships between treatments and outcomes is provided by mediation and moderation approaches (Breitborde et al., 2010). Because the mediator is an intermediary in the chain of causes, they are useful in explaining relationships between two variables. This clarifies "how" the three (3) variables are related to one another. Moderators take into account the particular circumstances in which two variables are associated. As the moderator's levels vary, the two variables' relationship changes. This clarifies "when and under what circumstances" the result of a variable may be maximised. Clinicians may fine-tune therapies using the crucial evidence provided by mediators and moderators.
Significance: This longitudinal, second-generation design pilot study investigates the relationships between sleep, physical activity, and arthritis tiredness. Since there are many contributing factors to arthritis tiredness, this research (third (3rd) variable design) focuses on two variables and how they interact to affect the result of arthritis fatigue. The effects of treatment (e.g., medicine) alone on arthritis tiredness are insufficient (Nikolaus et al., 2013). In the current treatment of arthritis, cognitive behavioural strategies, such as health promotion to encourage physical activity, might be targeted to reduce weariness. Understanding the relationship between physical activity, sleep, and arthritis tiredness is important because it allows doctors to modify current therapies to increase their potency and customise interventions. The information from this research is useful for the design of future, more extensive longitudinal clinical studies to examine the impact of exercise and sleep on arthritis tiredness. The study's findings also shed light on tiredness treatment strategies that could be appropriate in situations including fibromyalgia, autoimmune diseases, and cancer-related fatigue.
Purpose
This research looked at the relationships between sleep, physical exercise, and arthritis tiredness. In this study, the variables were investigated for their direct, mediating, and moderating impacts using Baron and Kenny's fundamental methodological framework (Baron & Kenny, 1986). The preliminary investigation found that physical exercise directly reduces arthritic tiredness. The second stage looked at how physical activity and sleep, the link between the variables, affect weariness. The mechanisms by which physical activity and/or sleep restrain or enhance the link to arthritic fatigue were then studied as moderating effects of the variables.
Aims
The study's primary goal was to see whether there was any correlation between arthritic tiredness symptoms and physical activity. Examining the role of sleep as a mediator of physical exercise on arthritic fatigue was the study's secondary goal. The third objective was to ascertain if sleep had a moderating impact on physical activity in the context of arthritic fatigue.
Primary Research Questions
Direct Effects:
1.0 What is the immediate impact of exercise on arthritis fatigue?
Inhibitory Effect:
2.0 Does sleep have a role in the connection between arthritic weariness and physical activity?
Modifying Impact:
3.0 Does sleep mitigate the wear-and-tear on arthritis caused by physical activity?
Theoretical Framework
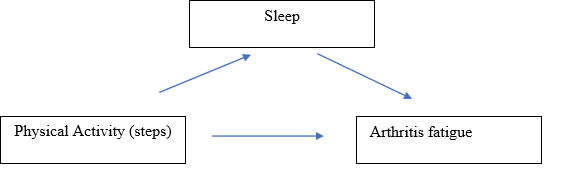
The conceptual and statistical mediation and moderation model serves as the theoretical foundation for this investigation (Baron & Kenny, 1986). Two models from the literature—the Theoretical Model of RA Weariness and the Biobehavioral Model of Fatigue in Osteoarthritis—were used to guide the selection of the variables for physical activity, sleep, and fatigue (Katz et al., 2016). Through a review of the literature, the Biobehavioral Model of Weariness in Osteoarthritis (Hackney et al. 2019) establishes the connection between fatigue, sleep quality, and physical activity. Based on a cross-sectional study of 158 RA patients, Theoretical Model of RA Weariness (Katz et al., 2016) establishes the association between physical activity sleep and sleep and their relationship to fatigue. Both Hackney and Katz mention a number of variables that have been linked to RA fatigue. But the goal of this research is to investigate the association between the arthritis-related controllable factors of weariness, physical activity, and sleep.
It was shown that physical inactivity had an indirect relationship with exhaustion, which was mediated by other factors including poor sleep (Katz et al., 2016). Other studies have not, however, shown any moderating effects of exercise or sleep on arthritis weariness. The study's remaining theoretical frameworks focus the investigation of the direct, mediated, and moderating effects of simple walking and sleep on arthritis tiredness.
1. What is the immediate impact of exercise on arthritis fatigue?
.png)
Definition of Terms
The Biobehavioral Model of Fatigue in Osteoarthritis (Hackney et al. 2019) and Theoretical Model of RA Fatigue served as the foundation for the study's independent and dependent variables (Katz et al., 2016). The operational definitions for each variable were improved and guided by a study of the relevant literature. The following sections provide explanations of the theoretical and practical definitions for each variable.
Demographic Variables
The survey gathered information on sex, race, ethnicity, education level, marital status, number of people living in the home, and current job.
Independent (predictors) variables
Physical activity and sleep were included as the study's independent variables. Simple walking was used to conceive exercise. Walking involves moving the feet in unison to propel the body forward at a slow to moderate speed. Walking is the movement a person does when engaging in regular activities as well as extra walking sessions. Simple walking may be done both indoors and outdoors and doesn't need any extra gear other than a pair of safe shoes. Simple walking was operationally defined using a step counter accelerometer that is readily available. Off-the-shelf technology is an economical method for measuring at home and offers a fair measurement over time. We utilised a Fitbit bracelet as an accelerometer to track daily steps during the research period.
Sleep was the second independent factor. The situation of being asleep is one in which the body and mind "usually recurs for many hours every night, during which the neurological system is generally passive, the eyelids are closed, the postural muscles are relaxed, and awareness is essentially suspended." Every night, people intentionally engage in sleep, which gives them time for rest and recovery (Cella et al., 2010).
The 8-item PROMIS Short Form v1.0 - Sleep Disturbance 8b (PROMIS SD-SF) was used to assess sleep (Yu et al., 2012). The PROMIS SD-SF evaluates self-reported impressions of the depth, quality, and restoration of sleep during the previous seven days. Greater sleep disruption or sleep-related impairment is correlated with higher scores. The amount of sleep each participant had was gauged at weeks 1, 4, and 6.
Dependent (Outcome) Variable
The study's dependent variable, arthritic tiredness, was assessed. The definition of fatigue is "an overpowering, crippling, and continuous feeling of weariness that reduces one's capacity to do everyday tasks, including the capacity to work efficiently and to function at one's typical level in family or social duties" (Cella et al., 2010). The PROMIS Weariness-Short Form was used to gauge study participant fatigue (Lai et al., 2011). The PROMIS F-SF is made up of eight questions that assess how much sleepiness you experienced last week as well as how much it interfered with your physical, emotional, and social activities. The available responses are listed on a Likert scale with 1 being never and 5 being always. We assessed participant tiredness at weeks 1, 4, and 6.
Summary
An annoying and frequent sign of arthritis is fatigue. Numerous cross-sectional approaches have been used to study arthritis fatigue in great detail. There is ample evidence that arthritic fatigue is a complex problem, and that the factors of physical activity, sleep, and weariness are related to one another. Other co-morbidities might be affected by controllable factors including physical exercise and sleep.
The link between physical activity, sleep, and weariness was investigated in this longitudinal research. The goal of this second-generation study is to comprehend how a third variable—sleep—operates and how its boundaries are defined. In order to evaluate the correlations and add on what is already known, this research adopted a mediation and moderation technique. This study is important in a number of ways. This study's longitudinal results expand upon what is known as a result of cross-sectional research. This study is important because it may help therapists better understand how physical activity and sleep impact, mediate, or reduce the effects of tiredness on clients and how to adapt therapies for them.
CHAPTER 2 - REVIEW OF LITERTURE
Purpose and Search Strategy
This section's goal is to discuss the most recent research on arthritis and the relevant factors of weariness, physical activity, and sleep. This part examines the potential for the conduct of this research project, the search technique, and a review of the literature on the relevant variables.
From August 2018 to February 2020, a thorough search of the literature was conducted to identify researches that investigate the connection between the factors of exhaustion, sleep, and physical activity. PubMed, EbscoHost (Science Citation Index, Academic Search Premier, CINAHL Complete, MEDLINE, PyschInfo, SPORTDiscus Direct), and Web of Science were the databases searched (WoS). The following primary MeSH search phrases were used to conduct searches across all of the databases on the list: "fatigue," "physical activity," "sleep problems," and "osteoarthritis" or "rheumatoid arthritis." Peer reviewed, clinical trial, present abstract, English language, and people were the search parameters for the article inclusion requirements. They were also published after 2000. Pharmaceutical trial, absence of an abstract, and abstract simply were the article rejection criteria. The relevancy and eligibility of the titles and abstracts were then carefully examined. 12 items were found after doing the search. For information, see table 1.
Table 1
Search Strategy
.png)
Arthritis
A severe illness called arthritis affects over 54 million individuals in the US in different forms (Barbour et al., 2017). According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), arthritis is a disorder that affects the joints, tissues surrounding the joints, and connective tissues, resulting in joint pain, stiffness, and deformity. The symptoms of arthritis make it more difficult to move, making it the primary cause of disability (CDC, 2009). By 2040, it is anticipated that more than 78 million individuals would have arthritis (Hootman et al., 2016).
Over 100 different forms of arthritis exist (CDC, 2019). Rheumatoid arthritis and osteoarthritis (OA) are the two types of arthritis that are most common (RA). Although the pathogenesis of arthritis is different, the disease burden is same (Chua et al., 2019). OA and RA have long-term repercussions that include joint pain, joint deformity, and disability (Hootman et al., 2012). It is believed that both forms of arthritis cause inflammation (Arthritis Foundation, 2020; Hackney et al., 2019).
The most prevalent kind of arthritis, osteoarthritis, affects 30 million Americans over 65, mostly women (Hawker, 2019). When the cartilage between bones deteriorates from osteoarthritis, it causes the joints to become painful, swollen, and difficult to move (Arthritis Foundation, 2020). Age, sex, previous injury, weight, and heredity are all risk factors for osteoarthritis (Sakalauskiene & Jauniskiene, 2010). According to Ashford and Williard (2014), osteoarthritis is not a normal part of ageing and its symptoms may be treated to stop the condition from becoming worse and causing impairment (Hootman et al., 2012) The second most prevalent kind of arthritis is rheumatoid arthritis (RA). The body assaults healthy tissues and cells since it is an autoimmune illness (National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), 2014). Chronic inflammation brought on by RA results in loss of function in the organs and joints as well as pain, edoema, and stiffness (NIAMS, 2017). Approximately 1.5 million individuals in the US suffer with RA (Hootman et al., 2016). According to Scott et al. (2010), the usual age of onset is between 40 and 60 years, and women are more likely than males to have RA (NIAMS, 2017).
Current Arthritis Treatment Overview and Role of Nursing
The management of the disease process, enhancing cognitive behavioural processes, and addressing personal difficulties and individual requirements are the three main areas under which arthritis therapy approaches may be divided (Hewlett et al., 2011). Each of the three tactics need for nursing knowledge. Nursing care influences illness management, makes use of cognitive behavioural strategies, and takes part in the treatment of individualised problems such co-morbidities. The overview of arthritis therapy and the function of nursing are both discussed in this section.
A range of medicinal therapies may be used to manage the arthritis disease process. Joint replacement surgery can be necessary for treatment (Hawker, 2019). In certain circumstances, drugs are utilised to reduce the inflammatory response and restrict the progression of the illness (Scott et al., 2010). The relationship between inflammation and disease activity in arthritis is largely unclear (Hackney et al., 2019; Matura et al., 2018). Not all of the symptoms that patients experience are entirely addressed by medical treatment (Hootman et al., 2012; Walter et al., 2018). Patients with arthritis benefit from medical therapies in terms of pain reduction and improvement. Interventions in cognitive behaviour show promise because they provide additional or alternative forms of therapy.
The interactions between ideas, emotions, behaviours, and symptoms are reflected in cognitive behavioural therapies (Hewlett et al., 2011). Pain and tiredness symptoms have improved as a result of applying cognitive behavioral techniques to manage the complete person and encourage behaviour change (Ferwerda et al., 2017). In sedentary arthritis patients, interventions that reduced sitting time increased activity levels, enhanced physical function, and decreased levels of weariness (Thomsen et al., 2017). Changes in behavior, such as increasing physical exercise for health reasons, may reduce tiredness symptoms and boost function by 40%. (Kelley et al., 2011). Interventions using cognitive behavior to encourage a healthy lifestyle may also be tailored to the unique difficulties each client with arthritis experiences.
The third step in treating arthritis entails controlling each patient's particular personal circumstances. Managing co-morbidities is part of providing care for persons with arthritis (Hewlett et al., 2011). For arthritis patients, co-morbidities are a challenge. Arthritis, and the resulting decrease in physical activity, makes it harder to manage the chronic conditions of heart disease and obesity. About half of all adults with arthritis have been diagnosed with heart disease, and one third have been diagnosed with obesity (Chua et al., 2019; Tournadre et al., 2018).
In order to effectively treat arthritis, medical therapy of the condition must be combined with cognitive behavioral therapies to encourage a healthy lifestyle and personal difficulties specific to the patient, such as co-morbidities (Hewlett et al., 2011). Professionally speaking, nurses are qualified to help in each of these situations. Clients benefit from nurses' knowledge in sickness treatment and health promotion. This research contributes to our understanding of the interaction between sleep and physical activity for health promotion and offers further details on how these activities contribute to arthritic fatigue.
Fatigue in Arthritis
It has been shown that fatigue levels are comparable across various forms of arthritis (Cross et al., 2008). The majority of people with severe arthritic tiredness are women, unemployed people, and those who don't exercise too much (Tournadre et al., 2018). Patients with arthritis state that weariness is their top priority and biggest worry, however healthcare professionals often ignore this fact (Hewlett et al., 2005; Power et al., 2008). Patients' top concerns revolve on arthritis weariness, which is persistent and common.
Physical Activity and Fatigue
Numerous physical activity/exercise therapies, including yoga, low-impact aerobics, dynamic strength training, and pool-based therapy, have been proven to be effective in reducing tiredness (Cramp, Hewlett, et al., 2013; Katz et al., 2018). By enhancing a person's aerobic and functional capacity, physical exercise therapies lessen tiredness and hence require less effort to do everyday activities (Katz, 2017).
According to Kelley, Kelley, and Callahan's (2018) research, aerobic exercise greatly reduces the symptoms of weariness. Katz and colleagues (2018) also noted that a walking intervention that increased physical activity over a twenty-one-week period helped arthritis patients feel less worn out. These physical activity programmes also had a somewhat significant impact, according to two recent meta-analysis studies (Cramp, Berry, et al., 2013; Rongen-van Dartel et al., 2016). Numerous types of physical exercise seem to help with arthritic weariness.
Walking has been recognised a fair kind of exercise when determining which physical activity is best for those with arthritis (Baxter et al., 2016). Walking involves moving the feet in unison to propel the body forward at a slow to moderate speed. The demands of patients with tiredness, who often find it difficult to go to locations outside of their homes for exercise training, may be met by walking, which is simple to learn and requires minimal expert direction and equipment. Accelerometers may be used to count steps as a tool to quantify exercise; for instance, Fitbit has been shown to be reliable for recording walking as exercise in fragile elderly persons with slow gaits (Case et al., 2015; Le Masurier & Tudor-Locke, 2003). (Paul et al., 2015).
Sleeping Quality and Arthritis Fatigue
Most arthritis sufferers complain about poor sleep quality (Fertelli & Tuncay, 2019; Goes et al., 2017). A link exists between insufficient sleep and greater than average levels of reported weariness in older persons with arthritis (Hawker et al., 2010). Some research indicate that increasing physical exercise may help people sleep better (Dolezal et al., 2017). Higher levels of physical exercise among arthritis patients result in greater overall sleep time (McKenna et al., 2018). This implies a connection between exercise and sleep.
Relationship between Arthritis Fatigue, Physical Activity and Sleep
It is difficult to assess the mechanisms underlying the relationship between arthritis fatigue, physical activity, and sleep because there is little research that: 1) considers all the variables simultaneously; 2) employs uniform measurement tools; and 3) is behaviorally based rather than based on a drug trial. The studies that incorporate cross-sectional and single randomised controlled trial (RCT) designs and include at least one of all the relevant variables are expanded upon in this section.
In older individuals, increasing physical activity is linked to better sleep and fewer signs of weariness (Christie et al., 2016). In a research looking at the connection between physical activity, sleep quality, and weariness in persons living in communities, 22 older adults (aged 65-81) took part. This research implies a connection between the factors, however the sample size was modest, the study lasted more than seven days, and the group was made up of healthy individuals rather than those with arthritis.
Loppenthin et al. (2015a, 2015b) looked at a community of arthritis patients in a large research (n=384) to investigate the associations between arthritis, physical activity, sleep, and other characteristics. These research' results indicated that physical exercise reduces exhaustion and that sleep quality and weariness are related (Loppenthin, Esbensen, Jennum, et al., 2015; Loppenthin, Esbensen, Ostergaard, et al., 2015). Although physical activity, weariness, and sleep are discussed in these research, the links between the three variables are not explicitly stated. The cross-sectional nature of these investigations further restricts their scope.
Rongen-van Dartel uncovered factors that support the association between arthritic tiredness, physical activity, and sleep (2016). Poor sleep and decreased physical performance were shown to be directly connected to increased degrees of tiredness in this research of 228 arthritis patients (Rongen-van Dartel et al., 2016). This study suggests a link between the variables, even if the cross-sectional design does not specify the direction of the association.
Indirect links between physical activity and exhaustion were discovered, which were mediated by insufficient sleep (Katz et al., 2016). This study examined 158 arthritis patients to identify factors related to weariness. This research reveals a link between the variables, although its cross-sectional methodology has certain limitations.
Through its connection to pain and exhaustion, sleep quality has an indirect impact on functional capacity, which includes walking. Fatigue and pain were shown to be mediators of the association between sleep quality and disability in a cross-sectional study of 162 people with arthritis (Luyster et al., 2011). The study has limitations in that the factors of interest are not explicitly addressed, despite the fact that it offers some information. The cross-sectional design makes it difficult to determine the cause, scope, or size of the mediators between sleep quality and impairment.
The literature contains one important piece of study. Durcan et al. (2014) used a randomised control trial research design to assess the impact of exercise on sleep efficiency and weariness. Following the baseline evaluation, experts created a customised 12-week workout programme with follow-up scheduled every three weeks. The exercise regimen included a number of therapeutic modalities, such as strength training, range-of-motion exercises, and walking. There were 38 participants in the control group who got standard treatment and information on the advantages of exercise for RA, and 40 patients in the intervention group who received these same services. According to Durcan et al. (2014), the physical activity intervention enhanced sleep quality and feelings of exhaustion since there was a statistically significant improvement for the intervention group in both areas (p = 0.04).
This research does have certain restrictions, however. Experts (a doctor and a physiotherapist) assessed the baseline evaluations to develop a customised 12-week programme with follow-up every three weeks for the expert and time-consuming exercise intervention. A significant amount of resources were also needed for a number of therapeutic modalities included in the intervention, such as weight training, range of motion exercises, and walking. Simple interventions like walking could be enough to have this impact.
Opportunity for Research: The Gap
The Disk implications of the earlier study designs and findings provide a chance to increase the body of research on sleep, arthritis fatigue, and physical activity. According to the research, these factors have been linked to an increased risk of arthritis in people. However, the majority of the research only assesses two of the three important characteristics. Since the majority of the researches examining this link have been cross-sectional, no additional conclusions can be drawn than correlations. The variety of assessment techniques employed in the literature on tiredness, exercise, and sleep is another difficult aspect (McKenna et al., 2017). Comparing the study's findings becomes challenging as a consequence. Physical activity, weariness, and sleep may not be related in a straightforward linear manner. It has not been thoroughly explored how and when the variables interact.
Theoretical Framework: Mediation and Moderation Models
The Theoretical Model of RA Fatigue and the Biobehavioral Model of Fatigue in Osteoarthritis (Hackney et al.) served as the foundation for the development of the theoretical framework in this research (Katz et al., 2016). The mediation moderation model serves as the study's general framework (Baron & Kenny, 1986). The planned study looked at the connection between exercise, arthritic tiredness, and sleep quality.
A comprehensive review was used to create the Biobehavioral Model of Fatigue in Osteoarthritis (Hackney et al., 2019). The correlates of tiredness were built into a model by the authors. The two behavioural components that are recognised as having a direct impact on weariness are physical activity and sleep quality. This model's lack of scientific validation is one of its drawbacks.
The Theoretical Model of RA Fatigue served as the study's second model (Katz et al., 2016). The research utilised data from a study that investigated the causes of tiredness in a sample of 158 people with rheumatoid arthritis. The results showed a statistically significant link between weariness, insufficient sleep, and physical inactivity. Poor sleep acted as a mediator in the link between physical inactivity and weariness, according to a mediation study (Katz et al., 2016). The cross-sectional form of the research and the emphasis on inactivity as opposed to activity are its weaknesses.
But the connections that have been made help us understand the correlations that exist between these factors, allowing for further investigation.
The work of Baron and Kenny serves as the foundation for the general framework that supports the conceptual and statistical technique of mediation and moderation (1986). To represent the interaction between variables outside of the discovery of a causal link, mediation and moderation are two separate ideas and uses (Baron & Kenny, 1986). Here, the conceptual paradigm of mediation and moderation is briefly addressed; Chapter 3 describes the statistical approach.
The literature study reveals connections between arthritis tiredness and may be regarded as first generation research. The evaluations imply that second-generation research focused on "how," "why," "for whom," and "under what conditions" is the next stage in the development of this knowledge (Breitborde et al., 2010). These second-generation research questions may be asked using the framework provided by mediator and moderator methods.
You may think of mediation as the "how" and "why" of variables. Finding a mediator in a causal link helps to understand the interaction between the independent and dependent variables. The mediator is crucial because, if it is discovered, it acts as an intermediary in the chain of events (Breitborde et al., 2010; MacKinnon & Luecken, 2008). Only in situations where there is a causal link may a mediator be present. This study's primary goal is to establish if physical exercise and arthritis tiredness are causally related. If such is the case, the second goal of this research is to ascertain how sleep fits into the chain of events that leads from physical activity to arthritic weariness.
Moderators take into account the particular circumstances in which two variables are associated.Moderators explain how the variables "when" and "under what circumstances" are connected. As the moderator level varies, the relationship between the independent and dependent variables changes (MacKinnon and Lueken, 2008). The investigation of sleep and physical activity, both alone and together, and their impact on arthritic tiredness is the third and final goal.
Summary
An incapacitating chronic illness, arthritis. Treatment for arthritis involves a variety of approaches, including medical management of the disease process (such as surgery or medical intervention), behavioural elements (such as promoting physical activity and sleep), and other personal/individual requirements including co-morbidities. Opportunities for behaviour are promising and fit easily within nursing's objectives and actions.
Using a mediation moderation approach, this study analyses the relevant variables—physical activity, arthritis tiredness, and sleep—and investigates their connection. Additionally, this study makes use of PROMIS standard measuring techniques so that other PROMIS researchers may expand on the findings (Bartlett et al., 2015).
Understanding the connection between physical activity, arthritic tiredness, and sleep offers the chance to enhance clinical care and research efforts in nursing and medicine.
CHAPTER 3 - METHODS
Introduction
This pilot study's goal was to investigate the connection between exercise, arthritic tiredness, and sleep. The goal of this research is to investigate how sleep, over time, affects the link between physical activity and arthritic tiredness. The research design, sample, intervention, tools, processes, and data analysis are all covered in this chapter.
Study Design
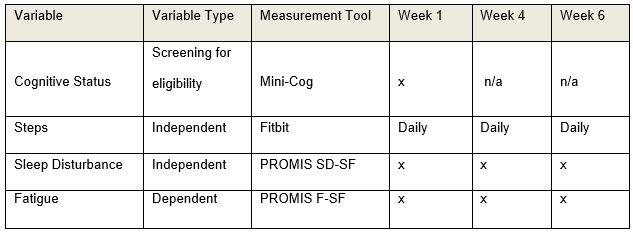
Investigation Design An experimental, long-term repeated measurements design was used in this study. Three outcomes were measured for participants (n=24): daily steps, disturbed sleep, and exhaustion. Self-reported questionnaires and accelerometer data were used to gather the results at the baseline, week four, and week six.
Sample
The research, which was carried out in many rural New England villages, was representative of the region's existing elder resident population. The Foundation of State Nurses, a State Council on Aging, a senior facility, and a YMCA in western Massachusetts were used to find participants. The sample included 24 persons with moderate tiredness, ranging in age from 50 to 86. 24 individuals were selected based on the advice that 10-15 per group is sufficient when the goal of the research is to investigate the impact of the pilot intervention, despite the fact that sample size calculation was not done due to the pilot nature of the study (Hertzog, 2008).
1) Participants in the study had to be 50 or older. 2) Osteoarthritis or rheumatoid arthritis self-reported by the patient, and 3) PROMIS Tiredness Short Form v1.0 -Fatigue 8a (PROMIS F-SF) score of more than mild fatigue (Lai et al., 2011). Inability to walk or the presence of a condition that would prevent it (such as a foot deformity, surgery on a lower extremity joint within the previous six months, a stroke, severe chronic obstructive pulmonary disease, etc.) were the exclusion criteria. The Mini-Cog test also looked for overt delirium, dementia, or any conditions that indicated a decline in cognitive status (Borson et al., 2000).
Instruments
The capacity of the research participants' eligible study subjects to engage in cognitive testing was evaluated. Mini-Cog (Borson et al., 2005) was used to measure cognition. The Mini-Cog has two parts: a clock sketching test and a 3-item recall memory test. It is highly sensitive (76%) and specific (89%) and is not negatively affected by age, language, or education (Borson et al., 2005). (Borson et al., 2003).
Steps were recorded using a Fitbit accelerometer worn on a bracelet. The Fitbit wristband was selected because it is accurate for recording step counts of fragile elderly persons with sluggish gaits and has a long battery life of up to 6 months for simple wear without recharging (Case et al., 2015). The built-in Fitbit app was utilised to monitor and log daily steps taken. The PROMIS F-SF was used to quantify participant weariness (Lai et al., 2011). The PROMIS F-SF is made up of eight questions that assess how much sleepiness you experienced last week as well as how much it interfered with your physical, emotional, and social activities. Options for responses are given on a Likert scale with 1 being never and 5 being always. Values might be anything from 8 to 40, with higher scores indicating more weariness. With Cronbach's alphas ranging from.72 to.88, PROMIS F-SF showed high dependability (Ameringer et al., 2016). The scale also demonstrated strong validity in populations with a range of ethnic and racial backgrounds (Ameringer et al., 2016); concurrent validity was supported by moderate to high correlations between PROMIS F-SF and the Multidimensional Fatigue Symptom Inventory-Short Form and between PROMIS F-SF and the Brief Fatigue Inventory (r =.70 to.85); and discriminant validity was supported by moderate correlations with other measures of related but unrelated constructs.The 8-item PROMIS Short Form v1.0 - Sleep Disruption 8b was used to assess sleep disturbance (PROMIS SD-SF). The PROMIS SD-SF evaluates self-reported impressions of the depth, quality, and restoration of sleep during the previous seven days. Greater sleep disruption or sleep-related impairment is correlated with higher scores. The scale demonstrated strong convergent-discriminant validity with high correlations with the Pittsburgh Sleep Quality Index (r=0.83-0.85) and low correlations with the Epworth Sleepiness Scale (r=0.25-0.30), as well as excellent internal consistency with Cronbach's alphas > 0.9 (Fogelberg et al., 2015). (Yu et al., 2011).
Procedures
The research received Institutional Review Board (IRB) clearance. A recruiting strategy was employed to concentrate on readily accessible hubs for arthritic customers. Focus areas included a state nursing research network, arthritis activity clubs, and arthritis support groups. Flyers that had been authorised by the IRB were distributed and put in provider care offices, senior centre bulletin boards, and fresh letters from the State Center for Aging. The participants' informed permission was sought after identifying those who could be interested. Then criteria for inclusion and exclusion were applied to the participants (see Sample).
The PI conducted an individual introduction session with all eligible participants (PhD student). The lesson included explanations of the study's methodology and goal, as well as guidelines for using an accelerometer. Participants completed the demographic survey at the conclusion of the session and received a Fitbit accelerometer to wear for six weeks. Participants had to show being able to comprehend the Fitbit screen's step counter and charging instructions. Additionally, everyone received an exercise journal to record their daily step totals before bed. Every two weeks, the participants were given self-addressed, stamped envelopes to submit their activity records in. A 6-week schedule of the study's activities, instructions for using the Fitbit, a copy of the permission form that had been signed, and the PI's contact information were given to the participants at the conclusion of the visit. Participants recorded their daily steps each night before bed in the weekly activity diary, which they completed each week. The PI contacted the participants once a week during the duration of the 6-week trial to check on any Fitbit issues and to address any study-related queries. Participants filled out the sleep disturbance and exhaustion questionnaires at the conclusion of weeks 1, 4, and 6. The list of variables and the timetable for data collection are shown in Table 2.
Data Collection Schedule
Data Analysis
For each of the relevant variables, descriptive statistics like mean, median, mode, and range were computed. To ascertain if randomization and normal distributions were adequate, data on participant characteristics and outcome variables were firstly examined. Using the models proposed by Baron and Kenny, the variables were also examined for a mediation and moderating impact of sleep (Baron & Kenny, 1986; Hayes, 2009; Zhao et al., 2010).
Sleep's meditative effects. The first stage in evaluating the direct effects of physical exercise on arthritic fatigue was to evaluate the connection of mediation.
1.0) What is the direct relationship between physical exercise and arthritic fatigue?
.png)
Mediation Analysis
The following two regression models were created at three different time periods, week 1, week 4, and week 6, to investigate the mediation impact of sleep. Look at Table 3.
Table 3
Regression Model for Mediation Analysis
.png)
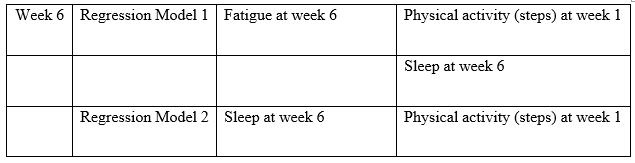
To determine if sleep mediates the connection between physical activity-induced arthritic fatigue and the following three conditions (Baron & Kenny, 1986).
1. There is a direct link between arthritic tiredness and physical activity (steps).
2. Physical activity (measured in steps) and sleep have a substantial link; and
2. When sleep is included into the regression, the impact of physical activity (steps) on arthritic tiredness will vanish (or at least lessen).
Moderation Effect of Sleep
3.0) Does sleep mitigate the impact of exercise on arthritic fatigue? Is the third research question.
The following regression model was created at three different time intervals, week 1, week 4, and week 6, to investigate the moderating impact of sleep:
Figure 6
Moderation Analysis
.png)
Table 4
Regression Model for Moderation Analysis
.png)
The statistical significance of the regression coefficient was examined in the regression models. If the result is significant, it suggests that sleep has a considerable moderating influence on the association between arthritic tiredness and physical activity (steps).
CHAPTER 4
REAULTS
Introduction
This pilot study's goal was to investigate the connection between exercise, arthritic tiredness, and sleep. This research was especially created to look at the mediation and moderating effects of sleep over time on the link between arthritic tiredness and physical activity. The findings for each of the three study topics are presented in this section.
Demographics and Descriptive Statistics
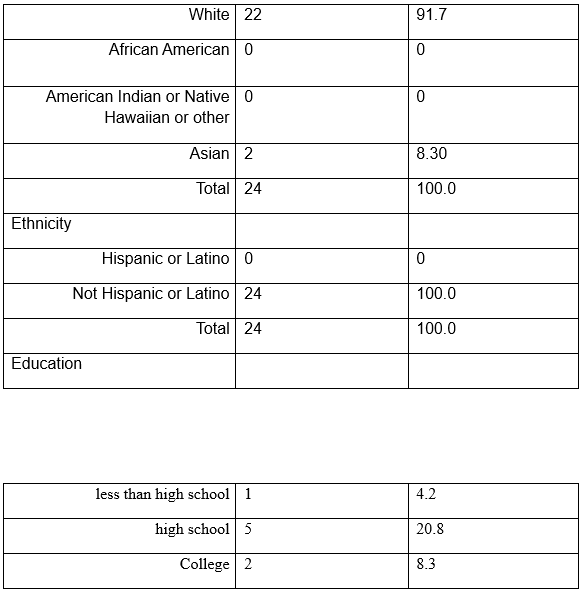
The 24 New Englanders that made up the research sample ranged in age from 55 to 86. The sample's ages were equally split throughout the three decades. Rheumatoid arthritis was reported by two thirds of the study group (n=16, 67%) and osteoarthritis by one third (n=8, 33%). Most research participants were married and lived with their spouses (n=16, 66.7%), female (n=18, 75%), and Caucasian (n=22, 92%). 25% (n=6) of the sample population had a high school diploma or less, according to the data. 18 people, or 75%, were college graduates or more. In Table 5, further descriptive information is included.
Table 5
Demographical Background
.png)
.png)
.png)

At weeks 1, 4, and 8, data were gathered for the independent and dependent variables.
6. The HealthMeasures Scoring Service evaluated the PROMIS Fatigue (F-SF) and PROMIS Sleep Disturbance (SD-SF) items. The service generated a T-score for each participant using de-identified survey data. With a mean of 50 and a standard deviation of 10, the T-score rescales the raw score into a standardised score. The PROMIS Fatigue (F-SF) values for weeks 1, 4, and 6 were used to determine the Cronbach's alpha, which varied from 0.94-0.97. For the PROMIS Sleep Disturbance (SD-SF) findings for weeks 1, 4, and 6, the Cronbach's alpha varied from 0.87 to 0.95. The number of steps was computed using the weekly average of each person's daily steps. Every measurement interval's minimum, maximum, mean, and standard deviation were computed for each variable. Table 6 displays these numbers.
Table 6
Descriptive Statistics for Independent and Dependent Variables (n=24)
.png)
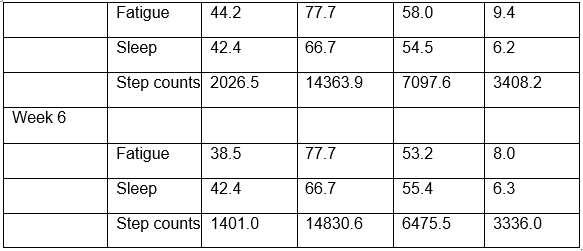
T-scores with an average score of 50 are created from fatigue and sleep scores.
Week 1 Results
What is the direct relationship between physical exercise and arthritic fatigue? A cross-sectional examination of the factors of physical activity, weariness, and sleep is done during week 1. According to the findings (=0.09, t=.42, p=.68), there is no connection between physical activity and arthritic weariness. See Table 7 and
.png)
Research Question #2. Does sleep modulate the impact of physical exercise on arthritic fatigue?
Two regression analyses linking physical activity, arthritic tiredness, and sleep are included in the Week 1 results (see Tables 8 and 9). The data demonstrated that step counts affect arthritic tiredness in both a direct (path coefficient=-.01) and indirect (path coefficient=-.18) manner, but that none of these effects is statistically significant. According to the findings, sleep does not act as a mediator between step counts and arthritis weariness. Look at Figure 5
Figure 8
Week 1 Cross-sectional Mediation Analysis
.png)
Table 8
Week 1 Cross-sectional Regression Results for Mediation Analysis
.png)
Research question #3. Does sleep lessen the impact of exercise on arthritic fatigue?
For sleep to moderate arthritic tiredness, there must be a considerable interaction between physical activity and sleep. There is no discernible moderating impact of sleep in week 1 according to the physical activity*sleep interaction data (=0.06, t=0.17, p=0.87). The link between physical exercise and weariness is not moderated by sleep.
Look at Table 9.
.png)
Figure 9
Week 1 Cross-sectional Moderation Analysis
.png)
Table 10
Week 1 Cross-sectional Regression Results Moderation Analysis
.png)
Week 4 results
Research question #1 what is the immediate impact of exercise on arthritis fatigue?
According to the Week 4 longitudinal data, physical activity and arthritic tiredness are significantly correlated (=-.19, t=-.40, p=.048). Look at Table 11 and Figure 7.
.png)
Research question #2 Does sleep operates as a mediator between the effects of exercise on arthritic fatigue?
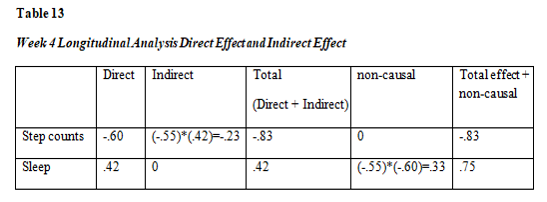
Two regression analyses relating physical activity, arthritic tiredness, and sleep are conducted in week four (see Table 12 and 13). The results demonstrated that exercise had a statistically significant direct (path coefficient=-.60) and indirect (path coefficient=-.23) impact on arthritis tiredness. The findings show that adding the sleep variable to the model raised the effect of physical activity from -.60 to -.83, indicating that sleep mediates the relationship between physical activity and arthritis tiredness. Look at Figure 8.
.png)
Research question #3 Does sleeps lessen the impact of exercise on arthritic fatigue?
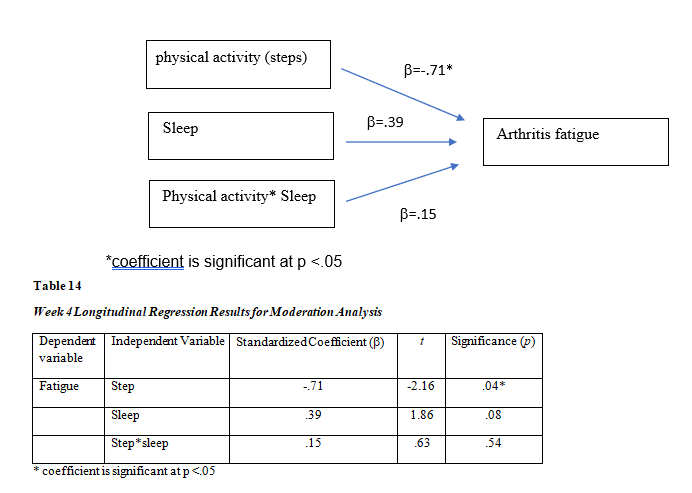
The interaction terms must be statistically significant in order to evaluate if sleep moderates the impact of physical activity on weariness. The physical activity*sleep interaction is not significant in the week 4 data (=.15, t=.63, p=0.54). Look at Figure 8. The association between physical activity and arthritic weariness is not moderated by sleep. Look at Table 13.
Physical activity and arthritic weariness, however, are significantly correlated ((=-.71, t=-2.16, p0.04).
Figure 12
Week 4 Longitudinal Moderation Analysis
Week 6 results
Research question #1 what is the immediate impact of exercise on arthritis fatigue?
There is no correlation between physical activity and arthritic tiredness, according to Week 6 longitudinal findings (=-.19, t=.60, p=.56). See Table 15 and Figure 10.
.png)
Research question #2 Does sleeps operate as a mediator between the effects of exercise on arthritic fatigue?
Two regression analyses linking physical activity, arthritic tiredness, and sleep are included in the data from week six (see Tables 16 and 17). The tables demonstrate a direct (path coefficient=-.61) and indirect (path coefficient=-.07) relationship between physical activity and arthritic tiredness, although only the direct relationship is significant. According to the findings, sleep is not a mediator of the connection between physical activity and arthritic tiredness. Look at figure 14.
.png)
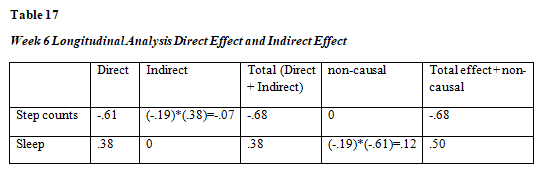
*Path coefficient is significant at p <.05
Research question #3 Does sleep lessen the exhaustion brought on by arthritis after exercise?
The interaction terms must be significant in week 6 data to evaluate if sleep moderates the impact of physical activity on weariness. Physical activity*sleep interaction is not significant in the week 6 data (=-0.003, t=-.01, p=.99). The association between physical activity and arthritic weariness is not moderated by sleep. Look at
Figure 15
.png)
CHAPTER 5
DISCUSSION
Study Overview
An extremely common symptom of arthritis in elderly persons is fatigue. This longitudinal pilot study's objectives were to investigate the link between physical activity and exhaustion as well as the mediating and moderating roles that sleep plays in this connection. The cross-sectional data at week 1 showed that there is no impact of sleep on arthritis tiredness in terms of mediation or moderation. The impact of physical activity rose from -.60 to -.83 in the longitudinal data at week 4, demonstrating that sleep mediates the relationship between physical activity and arthritic fatigue. The moderating effect of sleep, however, was not seen. The benefits of physical exercise on tiredness were neither moderated or mediated by sleep in the follow-up longitudinal data at week 6.
Mediation Effect of Sleep
Sleep's Mediation Effect Mediators provide light on the "how" and "why" of a causal relationship's third variable (Breitborde et al., 2010). According to the findings of this long-term investigation, sleep mediation started in week 4. The results are in line with those of earlier research by Katz (2016) and Luyster (2011), which found that tiredness symptoms were mediated by sleep. The standardised coefficients () for mediation had a considerable effect size (=-.83) and were statistically significant (Cohen, 1988). When sleep was included to the association between physical activity and arthritic tiredness in week 4, the impact size increased, going from -.60 to -.83. The results point to precise and distinct correlations between the three variables, with sleep playing a particular role in mediation.
Sleep did not operate as a mediator in the data from week 6 between physical activity and weariness. Even if the requirements for mediation were not satisfied, two of the three paths were important. Significant and having a modest impact size were the path coefficients between physical activity and sleep (=-0.61, t=-2.59, p=0.02) (Cohen, 1988).
Sleep and weariness were significantly correlated, however with a minor impact (=.38, t=2.18, p=0.04). The week 6 findings may indicate that the mediation of sleep on the link between physical activity and weariness may be time-limited when compared to the week 4 findings. The mediation effect was diminished after 4 weeks and vanished at week 6.
Comparison of Sleep Mediation in Cross-sectional vs. Longitudinal Results
The Theoretical Model of RA Fatigue by Katz et al. (2016) served as the foundation for this study's framework. Based on the results of their cross-sectional study, which included 158 arthritis patients, Katz et al. identified the probable explanatory factors connected with weariness. Katz et al. discovered that physical inactivity had an indirect relationship with tiredness, which was influenced by other factors including poor sleep. Some of the Katz et al. findings and the outcomes of this investigation were in agreement.
The longitudinal research found a substantial mediation impact of sleep but the cross-sectional study did not when comparing the mediation effect of sleep in the cross-sectional review at week 1 with the longitudinal review at week 4. Because the correlations were not explored longitudinally, the results may indicate that a cross-sectional approach may not always capture precise relationships, particularly cause-and-effect relationships between factors. A cross-sectional research design may not be the ideal method to find variable connections since mediation and moderation interactions are theoretically described as causal links between the variables (Barron & Kenny, 1986).
Moderation
Moderators provide light on the particular circumstances that exist between two closely related variables. In this research, it was expected that when the moderator variable (sleep) level changed, the connection between the independent variable (physical activity) and the dependent variable (fatigue) would also vary. In a cross-sectional investigation at week one or at the study intervals of week four or week six, this association was not discovered. The results imply that sleep may not operate as a moderator in the association between arthritic tiredness and physical activity.
Up until now, there hasn't been much knowledge on how sleep acts as a mediator between physical activity and weariness. In a recent research (n=481) of healthy teenagers, sleep quality was shown to mitigate the link between physical activity and weariness (Herring et al., 2018). There was a dose-response between physical exercise and reduced tiredness feelings in those who had trouble sleeping. The findings of this research do not agree with those of Herring et al. (2018). The research population was different and a cross-sectional design was adopted by Herring et al. (2018).
Strengths
There were a number of advantages to this research. The longitudinal research design with the mediation and moderation technique increased our understanding of how sleep affects the connection between physical activity and weariness. The research added to our knowledge of how sleep affects us over time, particularly the mediating effects of sleep in the fourth week. According to this research, a longitudinal design may disclose the precise mechanism by which sleep and physical exercise interact to affect arthritis tiredness.
The findings of this study back up the importance of second-generation research as a direction for nurse researchers. Finding a connection between variables is the goal of first-generation research. There are often several connections; for instance, arthritic tiredness has numerous correlations. How can a doctor begin to use this in patient care? Although first-generation research offers helpful cause-and-effect knowledge, its therapeutic use is limited (Guralnick, 1993). Second-generation study examines how connections' impacts function and the conditions' boundaries (MacKinnon & Luekin, 2008). For instance, this study's results showed that the association between physical activity and exhaustion is mediated by sleep. This reveals that the interaction takes time since the impact was not felt until week four. We also understand that the impact could only last for a short period of time since we did not detect it by week 6. This could affect the advice we provide to our customers.
The significance of practical behavioural techniques was stressed in this research. Sleep and physical exercise are behavioural elements that may be changed and have effects beyond mere exhaustion. With so many co-morbidities, physical exercise is a health promotion activity that is beneficial. Most individuals can engage in the affordable exercise of simple walking. Poor sleep is considered to interact with comorbid illnesses such pain, falls, cancer, and chronic heart failure as well as have an influence on these disorders (Onen & Onen, 2018). A health promotion activity that helps with tiredness and maybe other comorbidities is promoting excellent sleep hygiene.
The study's use of off-the-shelf technology, the Fitbit, gave researchers insight into instruments used in daily living. Fitbit, an accelerometer, is commonly sold at retail establishments. Globally, there are 100 million Fitbits in use, of which 28 million are active (Associated Press, 2019). The findings of this study may persuade other researchers to keep looking into how common arthritis sufferers may employ tools and remedies.
Limitations
The research has a number of drawbacks, including a small sample size, a straightforward design, effects from the seasons and holidays, and weather. The goal of this research was to serve as a pilot study. There were 24 older persons with arthritis fatigue in the sample. A larger sample size would provide more accurate and trustworthy findings.
The symptom of fatigue is multifaceted. There are over 100 factors that have been linked to arthritic tiredness in some way (Cramp, Hewlett, et al., 2013; Loppenthin, Esbensen, Jennum, et al., 2015; Loppenthin, Esbensen, Ostergaard, et al., 2015; Rongen-van Dartel et al., 2016). Two theoretical models of arthritic fatigue were used to guide the selection of the variables of physical activity and sleep in weariness (Hackney et al., 2019; Katz et al., 2016). In order to adequately represent the complexity of weariness, both models are multifactorial. The mediation and moderation methodology condensed the links to analyse arthritis tiredness in this research.
As a consequence, it's conceivable that our finding was influenced by other important factors. Both the Theoretical Model of RA Fatigue (Katz et al., 2016) and the Biobehavioral Model of Fatigue in Osteoarthritis (Hackney et al.) identify non-modifiable and modifiable variables that influence fatigue symptoms. The following variables are non-modifiable: age, sex, and illness status. In addition to physical activity and sleep, there are other controllable variables that affect weariness. Other modifiable characteristics that the theoretical models identify include depression, pain, and obesity. These other factors may have had an impact on the results even though they were not examined in this research. It is advised that future studies assess how they affect tiredness.
The use of wearable activity monitors, such the Fitbit, by older persons is now being studied. After two months, wearable activity trackers are no longer used by those over the age of 70. (Li et al., 2019). Researchers are still looking into why people stop using trackers, such how easy they are to wear and operate (Shin et al., 2019). This is consistent with mediation at 4 weeks and no mediation at 6 weeks, which may be attributed in part to the novelty of wearing the activity tracker for a brief length of time. Our research did not take into account potential changes in interest in straightforward walking over time.
In New England, the study recruitment was available all year round. The unpredictable New England weather has an influence on older adults who want to go on outdoor walks. Participants in the study were urged to choose secure walking routes. There were occasions when the weather made it impossible to go outside or to drive to a building where one could walk. One of the things that contributes to older adults taking less outside walks is the weather (Rantakokko & Wilkie, 2017). The recruiting period had an average of 46 inches of annual precipitation, 36 inches of annual snowfall, with average high and low temperatures between 82 and 13 degrees Fahrenheit (US Climate Data, 2019). Significant rains fell during 2019 (Page, 2019). One woman said, "I am not a duck," while describing her attitude about walking during a week of rain.
Participants also went on holidays and vacations, which would have reduced the amount of walking they could have done. Our sample included 14 participants, or 58 percent, who were retired. Participants visited family members during the course of the year in order to attend planned and unexpected events, holidays, and/or go on vacation away from their residences. The capacity to walk during part of the research period's weeks may have been hampered by travel time, whether by vehicle or aircraft, and unfamiliar surroundings.
Clinical Implications for Nursing
Complex care requirements must be met for older persons who are fatigued from arthritis. Three broad areas may be used to categorise arthritis therapy approaches: disease management, optimising cognitive behavioural processes, and client-specific demands (Hewlett et al., 2011). The last two of the categories are directly impacted by the study's results.
According to the study's conclusions, sleep gradually influences both physical activity and weariness. In order to increase the behaviorally modifiable parts of treatment, nurses will collaborate with clients to maximise the cognitive behavioural processes. Knowing that promoting physical exercise, such as brisk walking, might help with tiredness symptoms over time, nurses can encourage this behaviour. Additionally, nurses may encourage excellent sleep hygiene, such as a regular sleep pattern and sleep-enhancing activities before bed. The study's findings showed that sleep had a mediating role in the connection between physical activity and weariness, having a cumulative impact on easing sensations of fatigue.
Meeting the unique requirements of clients by treating co-morbidities is the study's second clinical application for nursing care. Comorbid conditions including heart disease, obesity, and diabetes affect older persons with arthritis fatigue at a significant rate (Barbour, 2017). Arthritis-related physical inactivity and the symptoms that go along with it do not aid in the treatment of other co-morbid illnesses. Promoting exercise, getting enough sleep, and reducing tiredness symptoms may give older adults more motivation to keep moving.
Further Research
The study's results recommend that future research concentrate on methods that might keep customers walking for extended periods of time. Patients with arthritis who get motivational counselling and SMS messages had their sitting time reduced (Thomsen et al., 2019). The additional significance of behaviour training in exercise therapies is a subject of growing research in osteoarthritis (Wellsandt and Golightly, 2018). Virtual peer groups and telecoaching are two additional approaches in the Chronic Obstructive Pulmonary Disease population that show potential for long-term promotion of exercise (Demeyer et al., 2017). It has been shown that using cognitive behavioural therapy may assist obese patients become more active over time (Grave et al., 2010). No of the approach, future research should incorporate measures and treatments that promote and encourage physical activity in arthritis patients.
Future studies should distinguish between various forms of arthritis and the severity of the disease process in study participants. Although osteoarthritis and rheumatoid arthritis have comparable illness burdens (Chua, 2019), comparing moderation analyses across different diagnostic types would need looking at a larger sample size. This would provide more clarity and give physicians the flexibility to customise advice for arthritic tiredness.
Also included in future study should be more complex statistical techniques like structured equation modelling (SEM). In order to choose the analytic routes, this research used Baron and Kenny's method to mediation and moderation using linear regression. SEM gives researchers the chance to look at the connections between several independent, dependent, and correlated variables in a single, substantial model. SEM also offers the benefit of being able to take measurement error into consideration (Zhao, 2009).
Conclusion
Using mediation and moderation approach, this longitudinal research investigated the effect of sleep on the connection between physical activity and arthritis tiredness. According to the study's findings, by week four, sleep acted as a bridge between physical activity and exhaustion. Sleep did not function as a mediator between physical activity and exhaustion at any other point throughout the 6-week research. In order to comprehend the operation and boundary features of a third variable—sleep—this study engaged in second-generation research. The findings imply that encouraging exercise and sleep may eventually lessen arthritis-related weariness. This study is important in a number of ways. Cross-sectional knowledge is expanded upon by the longitudinal results. The clinical community will be able to adjust their therapies to help people with arthritic fatigue as a result of this study, which is equally important. The results from week four point to a clear and correct association between the three variables, particularly the meditational function of sleep, which may help older people with arthritis fatigue and their healthcare professionals assure sleep promotion while reducing tiredness symptoms.
BIBLIOGRAPHY
.png)
.png)
.png)

- Assignment - Child Care
- Assignment - Mathematics
- Assignment - Accounting
- Assignment - Auditing
- Assignment - Biology
- Assignment - Law
- Assignment - Management
- Assignment - Nursing
- Assignment - Finance
- Assignment - Computer Science and IT
- Assignment - Humanities
- Assignment - Economics
- Assignment - Statistics
- Assignment - Architecture
- Assignment - Engineering
- Assignment - cookery
- Assignment - Marketing
- Case Study - Chemistry
- Case Study - Accounting
- Case Study - Law
- Case Study - Management
- Case Study - Nursing
- Case Study - Finance
- Case Study - Computer Science and IT
- Case Study - Engineering
- Case Study - Economics
- Case Study - Biology
- Case Study - Auditing
- Case Study - Marketing
- Case Study - Project Management
- Coursework - Diploma
- Coursework - Accounting
- Coursework - Auditing
- Coursework - Biology
- Coursework - Management
- Coursework - Nursing
- Coursework - Finance
- Coursework - Computer Science and IT
- Coursework - Engineering
- Coursework - Humanities
- Coursework - Child Care
- Coursework - Project Management
- Coursework - Economics
- Coursework - Cookery
- Coursework - Law
- Dissertation - Accounting
- Dissertation - Auditing
- Dissertation - Biology
- Dissertation - Law
- Dissertation - Management
- Dissertation - Nursing
- Dissertation - Finance
- Dissertation - Computer Science and IT
- Dissertation - Humanities
- Dissertation - Economics
- Essay - Politics
- Essay - Childcare
- Essay - Accounting
- Essay - Biology
- Essay - Law
- Essay - Management
- Essay - Nursing
- Essay - Computer Science and IT
- Essay - Humanities
- Essay - Economics
- Essay - Auditing
- Essay - Engineering
- Essay - Architecture
- Essay - Finance
- Essay - Science
- Essay - Marketing
- Programming - Computer Science and IT
- Reports - Management
- Reports - Computer Science and IT
- Reports - Project Management
- Reports - Marketing
- Reports - Nursing
- Reports - Engineering
- Reports - Accounting
- Reports - Humanities
- Reports - Finance
- Reports - Architecture
- Reports - Biology
- Reports - Economics
- Reports - Childcare
- Reports - Law
- Research - Accounting
- Research - Auditing
- Research - Biology
- Research - Law
- Research - Management
- Research - Nursing
- Research - Finance
- Research - Computer Science and IT
- Research - Science
- Research - Engineering
- Research - Humanities
- Research - Economics
- Research - Project Management
- Research - Statistics
- Research - Architecture
- Research - Marketing
- Thesis Writing - Computer Science and IT
- Thesis Writing - Engineering
- Thesis Writing - Biology
- Thesis Writing - Finance
- Thesis Writing - Humanities
- Thesis Writing - Auditing
- Thesis Writing - Economics
- Thesis Writing - Law
- Thesis Writing - Nursing
- Thesis Writing - Accounting
- Thesis Writing - Architecture

.png)
~5.png)
.png)
~1.png)



















































.png)






