Evaluating Knowledge and Attitudes of Undergraduate Nursing Students Regarding Pain Management Assignment Sample
Chapter 1
Introduction
Given that millions of cancer patients experience chronic pain from illness, surgery, or trauma on a daily basis, unmanaged pain has come to the attention of many healthcare professionals in the oncology environment (Deandrea, Montanari, Moja & Apolone, 2008). This approach of nursing assignment has greatly advanced the development of evidence-based recommendations and research on the management of pain in cancer patients with both acute and chronic illnesses (National Comprehensive Cancer Network, 2010). The number of cancer patients experiencing unrelieved pain has been increasing exponentially despite these recent advancements (American Cancer Society, 2009). In fact, the problem has gotten so bad that pain has been designated as the fifth vital sign (American Academy of Pain Management, n.d.).
Unmanaged pain has been highlighted as a significant barrier to the overall care of cancer patients in the oncology population. According to estimates, more than 75% of cancer patients will experience breakthrough pain at some point over the course of their illness (American Pain Foundation, 2010).
Cancer pain, which can result from a variety of problems, severely reduces the quality of life for both patients and their carers (American Cancer Society, 2009). As a result, the Ad Hoc Committee on Cancer Pain of the American Society of Clinical Oncology (ASCO) said in 1992 that 70% of cancer patients would feel significant pain at some time in the course of their disease, with more than 80% receiving poor treatment. The committee therefore created crucial and urgent guidelines for better pain management in the oncology population by encouraging better pain assessment and treatment abilities as well as formal training and education of healthcare professionals about pain management (ASCO, 1992). The Agency for Healthcare Research and Quality likewise revised its 1994 guidelines for the treatment of cancer pain in 2001. Due to the widespread belief that many cancer patients are still receiving inefficient pain relief methods, this was also intended to improve cancer pain management skills. Nevertheless, despite the existence of all these recommendations for efficiently managing cancer patients' pain, uncontrolled pain is still a common issue.
Problem Statement
Pain actually affects all psychophysiological levels and practically all facets of a patient's life, including interpersonal interactions, everyday living activities, and the ability to execute their job. As a result of incapacity, lost workdays, and decreased production, pain is estimated to have a 90 billion dollar economic impact (Turks, 2006). The American Nurses Association (ANA) states that nurses must keep up-to-date on pain assessment and management (ANA, 2001).
So, if pain is the most prevalent reason people seek medical attention, why is it the condition that is treated the worst? Many professionals in the area believe that the inexperience of nurses and doctors is one factor in why people continue to needlessly suffer from incorrect pain treatment (Lasch, Greenhill, Wilkes, Carr, Lee, & Blanchard, 2002). Many medical personnel are unprepared and unmotivated to manage pain adequately, which causes many patients to have a lower quality of life (American Cancer Society, 2009). This ignorance starts with fundamental educational initiatives.
A review of the literature over the past few years has revealed that neither the medical nor the nursing curricula contain enough educational material to adequately equip students to handle their patients' pain demands. This problem could be caused by the fact that nursing professors are not effectively equipped to teach students about pain management, either because they lack understanding in this area or because they do not stay up to date with current evidence-based methods (Ferrell, McGuire, & Donovan, 1993). Additionally, this educational shortcoming may have influenced nurses' unfavourable attitudes about patients seeking pain relief as many of these poorly prepared nursing students went on to become nurses. For instance, many nurses lacked appropriate knowledge of the dosages, applications, and fundamental mechanisms of action of many drugs, as well as other pain management techniques (Lasch, et al., 2002).
Few studies have examined baccalaureate nursing students' skills and attitudes in successfully managing the pain of their patients with reference to the undergraduate nursing programme (Diekmann & Wassem, 1991). Due to a lack of material in their curriculum, these children have also demonstrated a profound lack of knowledge. This curricular gap could be caused by out-of-date textbook content, poor instruction by teachers due to their own ignorance of the subject, or a combination of these factors (Ferrell et al., 1993). The combined impacts of these have a significant negative impact on baccalaureate nursing students' ability to effectively manage pain. Since there are few studies that focus on this topic and many students still struggle to manage their patients' pain successfully, the goal of this study was to investigate the knowledge and attitudes of undergraduate students regarding pain management.
Assumptions
In this study, there are two presumptions made:
1. The majority of cancer patients do not effectively control their pain.
2. By instructing nursing students, pain management will be improved.
Research Questions
The following research queries are addressed in this study:
1. What amount of expertise in pain management do baccalaureate-level nursing students have?
2. How do nursing students feel about treating pain in cancer patients?
3. Is there a connection between baccalaureate students' views and knowledge about how to treat pain in cancer patients?
Definition of Terms
The following terms are defined for this study's purposes:
1. Pain management: According to the American Pain Society Quality of Care Task Force, (2005) any interventions used to comprehend, lessen, and explain the causes of pain are included in pain management.
2. Pain: According to the American Academy of Pain Management (n.d.), pain is a complex combination of emotions, culture, experience, spirit, and sensation that is transmitted through the nervous system and sensed by the body. In other words, each patient who experiences pain is an individual with their own complicated psychological and physical experience.
3. Knowledge: Understanding of facts, concepts, and information acquired through instruction, experience, and learning for a specific purpose (Merriam-Webster Online Dictionary, 2009).
4. Pain attitudes: A steadfast set of convictions and principles that influence how one responds or behaves in the presence of pain (McMillan, Tittle, Hagan, Laughlin, & Tabler, 2000).
Significance of Study
The purpose of this study was to shed light on baccalaureate nursing students' attitudes and understanding regarding pain treatment. Compared to other healthcare workers, nurses spend the majority of their time at the patient's bedside, hence they are crucial in the assessment and evaluation of pain. As a result, nurses must take the lead in bringing about change for better pain management results among patient populations. As a result, the patient suffers if nurses are inadequately trained and unprepared to properly relieve pain. For this reason, in order to enhance patient outcomes and effectively work with other healthcare professionals to treat pain, student nurses need to be well-educated and knowledgeable about pain and pain management.
Chapter II
Review of Literature
This chapter's goal is to give a review of the pertinent literature. The literature reveals a variety of barriers to efficient pain treatment and thereby shows their influence on patient outcomes. The lack of knowledge and the unfavourable attitudes of nurses, nursing professors, and baccalaureate nursing students are among the barriers that have been examined.
Knowledge About Pain Management
Effective pain treatment is being hindered most by nurses', nursing students', and nursing educators' lack of understanding (Chiu, Trinca, Lim, & Tuazon, 2003). In reality, the paucity of information described in early 1990s studies is still blatantly apparent in more current literature. For instance, deficiencies were found in students' responses to questions about the physiology of pain, assessment parameters, and distinguishing between addiction and tolerance and physical dependence, which were based on the criteria for minimally acceptable scores on many pain management questionnaires (Goodrich, 2006). Nurses should do a more thorough assessment of pain rather than just asking patients to rate it. Additionally, there were inconsistencies in the breadth of the material provided about pain in lectures. Most
According to surveys, more than 50% of nurses disagreed that patients were the best arbiters of their own suffering (Bernardi, Catania, Lambert, Tridello & Luzzani, 2007; Rieman, 2006). In fact, the majority of teachers and students admitted that they weren't sure whether to accept that the pain ratings provided by patients were correct. In these situations, nurses and students recorded lower pain scores than what was reported and gave patients lesser medication amounts (Goodrich, 2006; Lasch et al., 2002; McMillan et al, 2000).
Diekman and Wassem (1991) also showed how many nursing programmes had little to no instruction on managing cancer pain, leaving trainees ill-equipped to employ effective pain-relieving techniques. The necessity for more effective integration of pain management content into programme curricula was highlighted by Goodrich (2006), who found that there are various gaps in nursing education addressing pain management and students (both medical and nursing). Additionally, students mentioned that they were unprepared to carry out pain management responsibilities because they had received little to no knowledge about pain management (Ferrell et al., 1993; Lasch et al., 2002). As a result, Chiu and colleagues' 2003 study found that students from Australia and the Philippines also received insufficient pain instruction, which prevented them from properly addressing patients' suffering.
Only a small number of faculty members were found in past studies to have additional expertise in pain treatment. In fact, both academic staff and students said they lacked the knowledge necessary to apply pain management techniques, and supplemental treatments to successfully manage patients' pain. The faculty also concurred that teaching students about pain and cancer pain management would better prepare them for general practise (Ferrell et al., 1993;Lasch et al., 2002). In addition, Ferrell and colleagues (1993) reported that few educators had noticed changes in pain treatment techniques over the previous 20 years and were not aware that new regulations had been put in place to address patients' pain demands. Additionally, educators only minimally met students' demands for pain education in less than one-third of schools, teaching them about current research techniques in pain management (Lasch et al., 2002). The majority of research found that nursing educators must admit that their curriculum lack the requisite course material to adequately train their students on pain management (Goodrich, 2006; Ferrell et al., 1993; Lasch et al., 2002). As a result, curriculum changes are necessary to compel revaluation of current nursing programmes in order to support students' development of stronger pain management skills.
Additionally, a review of the literature revealed that students performed poorly on tests that asked about the administration, dosage, side effects, and mechanism of action of medications (Plaisance & Logan, 2006). Thus, despite improvements in pain management techniques, students showed a lack of pharmacology knowledge necessary for pain management. In order to better relieve pain, doctors, nurses, and students typically underused opioids (Lasch et al., 2002; McMillan et al., 2005). Data also showed that the majority of nurses were unaware that a mixture of medications might be used synergistically to relieve pain in a safe way, without patients experiencing respiratory depression, and they had sufficient knowledge of the World Health Organization pain ladder (Bernardi et al., 2007). Deficits in understanding the maximum dosage of some analgesics, calculating analgesic doses, as well as the mechanism of action and analgesic dosages for pain management, were generally observed in nurses and students' responses in classes (Goodrich, 2006; McMillan et al., 2005; McMillan et al., 2000). Additionally, nurses were not aware that continuous pain medications were more effective at controlling pain than waiting for patients to express it verbally (Bernardi et al., 2007). Additionally, faculty members lacked understanding of the opioids' ceiling effect, the distinction between addiction and physical dependency, and tolerance (Lasch et al., 2002). Since respiratory depression was also believed to be a serious adverse effect of opioid drugs if taken over a 24-hour period, statistically speaking, no changes in scores on the usage of opiates for pain management were seen (Bernardi et al., 2007; McMillan et al., 2005).
Overall, inadequate knowledge and negative attitudes were found to be resolved by continuous education. Nursing knowledge and attitudes can be improved by continuing education in intensive pain treatment, according to McMillan and colleagues' (2005) research. To deliver competent care and enhance patient outcomes, nurses must constantly stay up to date with current treatment guidelines (Diekmann et al., 1991). Although given that knowledge of pain management is a crucial component of effective nursing practise, more research is needed to address the integration of new educational modules in teaching nurses about pain and pain management. The majority of studies showed that there was little correlation between educational attainment and being better at managing pain (McMillan et al., 2005; Plaisance & Logan, 2006). In order to fully teach nursing students at all levels and themselves on how to manage pain in patients, instructors should apply novel educational methodologies. In fact, after receiving pain education, nurses, students, and teachers felt more competent in evaluating pain and applying the right measurements and techniques to successfully relieve it (Lasch et al., 2002; McMillan et al., 2005; Wilkes, Lasch, Lee, Greenhill & Chiri, 2003).
According to two studies, oncology nurses received more formal training on recommended pain management techniques than non-oncology nurses (McMillan et al., 2005; Rushton, Eggett & Sutherland, 2003). Data from both studies indicated that oncology-trained nurses provided better pain management results for patients and were more familiar with suggested practise guidelines than non-oncology nurses. However, neither group of nurses had a good understanding of the pharmacology of drugs used to treat cancer pain (Bernardi et al., 2007; McMillan et al., 2000).
Attitudes Toward Pain Management
Negative attitudes among healthcare workers and students are another another obstacle to efficient pain management. While most cancer patients do experience pain at some point during their illness, as many students and nurses correctly noted, very few thought that pain could be effectively relieved by medication or that it was appropriate for cancer patients to receive maximum tolerated treatment in order to become pain-free (Diekmann et al., 1991). Additionally, nurses believed that patients overestimated their level of pain, thus if a patient was cheery when visiting with the nurses, a lower pain rating was logged and the amount of pain medicine administered was decreased (McMillan et al., 2000).
Second obstacle, as most nurses would permit worries about addiction to influence their administration, pain ratings and drug dosages were also reduced in younger and older patients (McMillan et al., 2005; Rushton et al., 2003). When doctors prescribed patients 24-hour analgesics, a similar pattern was seen. The nurses would let their view that patients should feel agony before receiving medication affect how they gave out painkillers (Ferrell et al., 2003; McMillan et al., 2000). Students and teachers similarly voiced their concern that giving patients too much opioid medication might promote addiction, which was a big barrier to them giving patients analgesics (Lasch et al., 2002).
Inadequate nursing education was another barrier to developing good attitudes for pain care that worked. Nursing professors were more likely to pass along their own misperceptions about the physiology of pain and the pharmacology of drugs to students (who later became nurses) because they were insufficiently knowledgeable about the principles of pain treatment themselves (Ferrell et al., 1993; Lasch et al., 2002). It was also fascinating to observe that instructors and students were more prone to apply their own biases to patients if they were not well trained on pain treatment (Lasch et al., 2002). The data did not make it apparent, nevertheless, if oncology nurses were more sympathetic to patients who were in pain than non-oncology nurses.
Last but not least, the delivery of educational modules shown a significant improvement on attitude questions by nurses. Additionally, it was discovered that attitudes toward recording patients' pain had changed dramatically, demonstrating the need of education in pain management (McMillan et al., 2005).
Summary of Literature
In conclusion, a study of the empirical literature has revealed that the nursing curriculum lacks the instructional content to adequately equip its students to properly manage their patients' pain requirements. This problem can be brought on by the nursing faculty's own lack of readiness to teach students about pain management. Studies found that nursing instructors either lacked expertise in pain treatment or did not stay current with evidence-based procedures. Furthermore, since many of these ill-prepared nursing students went on to become nurses, this educational fault might have crept into their professional conduct, showing extremely negative attitudes and subpar pain management abilities. Therefore, more focus must be placed on teaching students about fundamental drug action processes, doses, and uses, as well as other pain management techniques.
Chapter III
Methods
The study's methodologies are detailed in this chapter. This comprises information about the sample's characteristics, such as the requirements for participation, the variables being studied, and a description of the measurement tools that were employed to gather the data. Additionally, the methods for gathering data and doing analyses are presented.
Sample
The target demographic for this study was undergraduate nursing students, and the sample comprised of willing undergraduate students at the University of South Florida who are currently pursuing a Bachelor of Science in Nursing (BSN) (USF). Being a senior BSN student at USF, enrolled in the Leadership and Management in Nursing course, being above the age of 18, being able to read and write English, and having taken undergraduate pharmacology and pathophysiology courses were the inclusion criteria for participation.Through the use of power analytical methods, the sample size was assessed. For a Pearson correlation, a sample size of 30 should produce significant findings with a power of 0.80 and an alpha set at 0.05.
Instruments
The Nurses' Attitude Survey (NAS), the Pain Management Principles Assessment Tool (PMPAT), and a demographic data questionnaire were the instruments used in this study. Both assessments were selected because they clearly distinguish between knowledge gaps and attitudinal barriers in pain management, making them suitable for the study.
Nurses’ Attitude Survey
The NAS, developed by McMillan and Tittle in 2000, consists of 25 items and measures attitudes toward pain management using a four-point Likert scale. Strongly disagree to strongly agree were the range of responses for the instrument, and each item's raw score varied from 1 to 4. The higher the score, the happier the nurses were. The study asked questions on administering analgesics on time, using opiates, assessing pain, its objectives, common myths, and non-pharmacologic pain management.
Reliability and Validity. Using Cronbach's alpha, a satisfactory level of internal consistency reliability (r=0.70) was discovered. When it was pre-tested and post-tested among nursing students, a significant difference (p.01) was found, which further supported its validity (McMillan et al., 2000).
Pain Management Principles Assessment Tool
The PMPAT consists of 31 multiple-choice questions with four possible answers. A test of pain management was intended for the questionnaire knowledge of physiology pharmacology, and the concepts of assessment and management as well as the characteristics of pain, such as addiction, physical dependence, and tolerance. The survey's scores ranged from 0 to 31, or 0 to 100%, with higher scores indicating more correctly answered questions.
Reliability and Validity.The tool's design was based on a framework from earlier research investigations attesting to the validity of its content. Using the pre- and post-test approach, the validity of the instrument was also examined before and after a three-hour pain management course was given to 28 nursing students. From the pre to post test, validity was determined to be highly significant (t=6.76, p0.01). Additionally, reliability was shown to be quite good (r=0.84, p=0.00) (McMillan et al., 2000).
Demographic Data Form
A demographic data form was also given to each participant to complete. The questionnaire asked about the respondent's age, gender, ethnicity, current semester of their BSN programme at USF, greatest level of schooling attained, work history, current employment status, and whether they had ever gotten any kind of pain management training.
Approval
Both the USF Institutional Review Board and the USF College of Nursing gave their approval for the study to be carried out, which allowed students to be approached about participating. The instructor of the Leadership and Management in nursing course was asked for approval before the surveys could be given to the students in class. Additionally, each participant received a letter outlining the goals of the research and the requirements for enrolment. The letter further emphasised that participation was voluntary and confidential, and that completing the questionnaires implied consent.
Procedures
Each student received a questionnaire during class time. The instructor of the Leadership and Management in nursing course was asked to leave the classroom before the questionnaires were given out, and the investigator stayed in the space to oversee the study, give out the surveys, and collect them. There was a brief summary of the study, stating that taking part had no risks or benefits for participants other than advancing the field of nursing research in the area of pain treatment. Additionally, students had the chance to ask any pertinent questions they might have had about the research. Students were also instructed to carefully study the provided instructions and complete their questionnaires on their own, without consulting any textbooks or other students.
Data Analysis
Descriptive statistics, such as frequencies, percentages, means, and standard deviations, were used to analyse the demographic data. Students' knowledge levels, attitudes toward pain management, and the relationship between knowledge and attitudes were examined using Microsoft Excel and the Statistical Package for Social Sciences (SPSS).
Means and standard deviations were calculated to address Research Question 1: What is the amount of knowledge of pain management principles possessed by nursing students at the bachelor level?
Means and standard deviations were determined to respond to Research Question 2: What are nursing students' perspectives toward pain treatment in the oncology patient?
The Pearson Correlations were performed to provide an answer to Research Question 3: Is there a significant association between knowledge and attitudes among bachelor students about pain treatment in cancer patients?
Chapter IV
Results, Discussion and Conclusions
This chapter includes the findings from questionnaires administered to University of South Florida undergraduate nursing students to ascertain their level of knowledge and current views regarding pain treatment. Discussion of the correlation between knowledge and attitude scores is also offered along with the results of the variables. This chapter also covers the study's limits, findings, and recommendations for further investigation.
Results
Sample
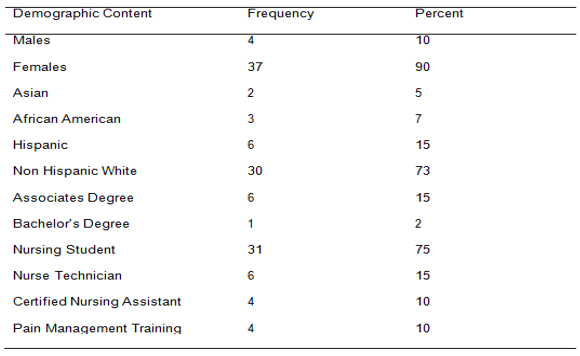
41 undergraduate students who are currently enrolled in their senior year of study for a Bachelor of Science in Nursing at the University of South Florida made up the sample for this study. 90% (n=37) of the 41 participants were women, while 10% (n=4) were men (Table 1). The age range of the students was 18 to 42 years, with a mean of 22.5 years. The bulk of participants—73%, or 30, were of non-Hispanic White ethnicity; the remaining participants were 7% (n=3) African Americans, 15% (n=6) Hispanics, and 5% (n=2) Asians (Table 1). According to study, the proportion of students with formal education ranged between 15% to prior to enrolling at USF, whereas 2% (n=1) had bachelor's degrees in subjects other than nursing (Table 1). The majority (75%, n=31) claimed to be full-time nursing students without jobs, while 15% (n=6) were employed as nurse technicians and 10% (n=4) were CNAs (Table 1). 20% (n=7) of students received training in pain management, compared to 80% (n=34) who received no training at all outside of what was provided in their nursing degree (Table 1).Table 1 shows the frequency and percentage of students by gender, ethnicity, and level of education, work experience, and pain management training.
Knowledge of Pain Management Principles
The PMPAT's raw results were tallied and analysed in order to respond to the first research question, which measured the knowledge of undergraduate nursing students on pain management (McMillan et al., 2000). Out of 31 items, the mean knowledge score was 19.4 (SD= 3.0), or 63%. According to the raw results, the 41 students' correct response rates ranged from 39% to 81%. Only 7 students, or 17% of the class, would have passed the pain management knowledge test if a passing score of 70% had been utilised, whereas 30 students, or 73%, would have scored between 50% and 75% and 4 students, or 10%, would have scored below 50%. (Table 2).
When the answers to the individual knowledge questions were analysed, it became clear that students performed poorly in the areas of pain physiology, the pharmacology of pain medications, the right time to take pain medication, the use of cutaneous stimulations as a measure of pain relief, and the primary goal of pain management practises, with scores of 39% or less. On the other hand, the concept of tolerance and patients as the most accurate and reliable judges of their own pain were the two subject areas where items obtained a score of 100%. Patients should be in charge of their own pain management plans, nurses should notify the doctor if a patient's pain worsens while taking the maximum amount of analgesics prescribed, and distraction as a pain management strategy were other categories in which ratings were 90% or above (Table 3).
.png)
Attitudes Toward Pain Management
The Nurses' Attitude Survey was used to gauge attitudes (NAS). Strongly disagree to strongly agree were the range of responses for the instrument, and each item's raw score varied from 1 to 4. The nurses' attitudes were more upbeat the higher their score. A mean score of 17.1 (SD=2.6) was calculated after the raw data from the attitude survey supplied to the sample was analysed, with a range of 48% to 88% of students having favourable views toward pain management.
According to the findings of an item analysis of the NAS, all 41 students (100%) agreed that continual evaluation of pain and drug efficacy is essential for efficient pain management. They also agreed that distraction and diversion could reduce patients' pain levels. Additionally, 95% of students concurred that patients may be reluctant to take painkillers owing to worries about using opioids, and that a nurse should consult a doctor if a patient's pain persists. Following this, 78% of respondents agreed that patients should be kept pain-free, and 71% agreed that cancer pain could be relieved with the proper anti-cancer medications, radiation therapy, and/or painkillers. These results were followed by 85% of respondents who agreed that a constant level of analgesic should be maintained in the blood to control pain effectively. Furthermore, 15% believed that patients in pain may withstand high doses of opioids without sedation or respiratory depression, and 39% felt that the cancer patient and family should have greater control over the schedule for analgesics than the medical professional (Table 4). Contrarily, 98% of students disagreed that a doctor's or nurse's assessment of a patient's pain is a more reliable indicator of that pain than the patient's self-report; 78% of students disagreed that patients should feel pain before receiving their next dose of painkillers; and 73% of students disagreed that patients receiving opioids round-the-clock for cancer pain are likely to develop addiction. In addition, 5% of students disagreed that patients taking 24/7 opioids are at risk for sedation and respiratory depression, while 29% of students thought cancer patients should receive pain medicine before the pain returns (Table 4).
Relationship Between Knowledge and Attitudes
A Pearson correlation between the total scores for knowledge and the total scores for attitudes was calculated to see if there is any association between knowledge and attitudes among bachelor students about pain management in cancer patients. The Pearson correlation coefficient of these two variables was r=0.33 (p=0.038), indicating a modest to moderate but significant degree of association.
.png)
.png)
Discussion
Sample
The convenience sample of 41 students from USF's undergraduate Bachelor of Science in Nursing programme responded, and this was enough to provide statistically significant and enough data for the study. The sample gave a clear cross-sectional impression of the USF nursing students that are enrolled in the programme right now. The findings from this study, however, may not be extrapolated to encompass the full population of undergraduate nursing students in Florida or the United States because the data was only obtained in one geographic location and had only a minimal representation from other ethnic groups. Additionally, there was relatively limited participation from minorities in this study because the sample was primarily made up of non-Hispanic Whites.
Since ethnicity and culture have an impact on knowledge and attitudes about pain management, the absence of participants from other ethnicities and cultures may have introduced bias into the data collection. The fact that all students were requested to participate rather than being randomly chosen was another study constraint, and it is unclear what impact this may have had on the data collected as well. The demographic data form's question about pain management training was incorrect since students might have taken it to indicate material covered in class rather than official training provided by a professional.
Knowledge of Pain Management Principles
On the knowledge test, the average score was 19.4 (SD=3.0), or 63%. Data revealed that nursing students have little understanding of how to treat pain. These results were comparable to those of Plaisance and Logan and McMillan and colleagues for nurses in 2000. (2006). McMillan and colleagues (2000) received a mean score of 18.8 (SD=2.9) or 61%, whereas Plaisance and Logan (2006) received an overall score of 64%. Because of this, nurses may not be learning important knowledge in their fundamental nursing programmes, even while the focus on pain remains a national priority.
Students demonstrated strength in some areas of the pain management knowledge test, despite the relatively low overall knowledge scores. For instance, 100% of the students correctly responded that patients are the best judges of their own pain, and 93% said that patients should be in charge of their own pain treatment regimen. This was in line with the results of McMillan and colleagues in 2000, who scored 96% and 81% respectively, but not with those of Bernardi and colleagues in 2007, where only 56% of nurses thought that patients were the most reliable judges of their own pain. This demonstrated that USF's present undergraduate programme does focus on pain management. This agrees well with the NAS, which found that 98% of students disagreed that a patient's self-report of pain is a more reliable indicator of pain than a doctor or nurse's evaluation of discomfort.
Most students were able to define tolerance correctly, describe naloxone's function, and employ a combination of analgesics to treat pain when it came to pharmacologic management. The results of McMillan and colleagues (2000), who reported an 89% score, were consistent with the fact that 100% of students could define tolerance. However, the threshold for distinguishing addiction from tolerance and dependence in the study by Goodrich (2005) was less than 80%. The finding that 93% of students agreed that patients should be in control of their pain management regiment was strength of this study. This result was significantly higher than the 81% score attained ten years earlier by McMillan and colleagues (2000).
Although the data analysis revealed few areas of competency, there were several areas where students' knowledge was significantly lacking.
Most of the inquiries in these categories concerned the physiology and pharmacology of pain. This aligns with earlier study investigations (Bernardi et al., 2007; Diekmann & Wassem, 1991; Ferrell et al., 1993; Goodrich 2005; McMillan et al., 2000; Plaisance and Logan, 2006). For instance, only 29% of students correctly identified that the best time to administer pain medication was before pain began, while only 37% of students were aware of the Gate Control Theory. C-fibers, which are responsible for dull, aching pain sensations, were also unknown to only 20% of students. In terms of pharmacology, just 14% of students were aware that oral administration of medications was the preferable method, 22% were aware that methadone was the opioid with the longest duration of action, and less than 60% were aware that meperidine caused toxicities to the central nervous system.
Less than 24% of students indicated that the main objective of pain management was complete pain relief, and less than 1% of cancer patients develop a drug addiction to painkillers, it was also reported. Additionally, there was a paucity of knowledge regarding the application of non-pharmacologic methods for treating pain of any intensity, such as cutaneous stimulation. Therefore, it is now evident why nurses struggle to manage patients' pain since students don't have a basic understanding of the physiology and pharmacology of pain. These findings imply that pain management issues will persist even after this new nursing generation enters the workforce.
Attitudes Toward Pain Management Principles
A mean score of 17.1 (SD=2.6) out of 25 was determined after the raw test scores from the sample were analysed. The views that many students have regarding pain management may be influenced by their lack of knowledge of the physiology of pain and the pharmacology of opioids. For instance, only 5% of students disagreed with the claim that patients receiving 24/7 opioids are more likely to experience sedation and respiratory depression. This finding is consistent with the low response rates for the question of whether patients in pain can tolerate high doses of opioids without experiencing sedation or respiratory depression. Because of this, students might be aware that increasing opioid doses are caused by opioid tolerance and do not always result in sedation and respiratory depression if they had a better understanding of the physiology of pain and the pharmacology of opioids. These findings, which were in line with earlier research, demonstrate that nurses and students haven't made much progress in this area over the past ten years.
It was also noteworthy that the sample of students who participated in the study were devoted to acting as ardent patient advocates and strongly believed that a patient's self-report of pain was more accurate than that estimated by a doctor or nurse. This was directly tied to the knowledge question, where all students unanimously agreed that patients were the greatest arbiters of their own pain. Only 39% of students believed that cancer patients and their families should have more say in the analgesic schedule than a medical practitioner, nevertheless.
Because cancer patients and their families spend the majority of their time managing chronic pain outside of the authority of doctors and nurses, the notion that they should have control over the analgesic regimen is erroneous.
As a result, we can see that nurses might adopt a more optimistic perspective on pain management if they gained a deeper understanding of the physiology of pain and the pharmacology of analgesics. Additionally, if students see the need of better educating patients on how to manage their own pain and giving patients and their families greater influence over their pain treatment programmes, they can create stronger interactions with their patients and, eventually, better patient outcomes.
Relationship between Knowledge and Attitudes
The data acquired showed that students who often scored highly on the knowledge test also scored highly on the attitude test, despite the Pearson correlation value (r=0.33, p=0.038) showing a weak to moderate association between knowledge and attitudes. The knowledge survey and attitude questionnaire share many items; however there seem to be some differences. As an illustration, students' knowledge of therapeutic levels appears to be lacking, despite their positive sentiments. In contrast to the 78% of students who disagreed that patients should feel discomfort before receiving the next dose of pain medication, only 29% of students correctly responded on the knowledge questionnaire that additional pain medication should be administered on an as-needed schedule before pain returns. This may suggest that students have trouble distinguishing between analgesics taken only when necessary and regimented analgesic treatment strategies.
The question of whether complete pain alleviation is a goal is another area where there appears to be ambiguity. Only 24% of students who responded to the knowledge survey thought that all patients should receive total pain relief, however 78% of students who responded to the attitude survey agreed that patients should be kept in a pain-free state. This could mean that even though students possessed the positive dispositions necessary for good pain management techniques, they lacked the information and justifications for why patients needed complete pain relief.
Another subject where pupils struggled was addiction. Only a tiny percentage (24%) realised that less than 1% of cancer patients developed a drug addiction to painkillers, even though 100% could describe tolerance appropriately. 73% of students who took the attitude test disagreed that cancer patients who get opioids continuously for pain relief are prone to develop an addiction. As a result, we can see that knowledge and attitude ratings on the topic of addiction appear to be unconnected. It's unclear how these nurses' inconsistent knowledge and attitude scores will ultimately affect how well they treat patients.
Conclusions
Despite the fact that pain management has been studied for many years, students' ignorance seems to be a key barrier to effective pain management techniques. Because this study revealed a lack of understanding and some unfavourable views, it is clear that more needs to be done to educate students on the physiology of pain and the pharmacology of analgesics. While students frequently possessed the optimistic outlook necessary for effective pain management approaches, they frequently lacked the underlying information and comprehension of why they were practising certain abilities. So it follows that training nurses and students is a positive step toward improving pain treatment techniques. Therefore, if we want to enhance the information that students receive regarding pain management, a modification in the current undergraduate curriculum is necessary. For this reason, learning about pharmacology, pain physiology, and gaining a better understanding of terms like tolerance, dependency, and addiction would help students become more knowledgeable and better able to care for patients with chronic pain. Therefore, it is essential that methods for improving student education be found if we are to pave the way for patients to receive better pain treatment techniques.
Implications for Nursing
The results of this study have various nursing-related ramifications. Future research on the knowledge and attitudes of undergraduate students on pain management should involve several educational institutions from various geographic regions and a diverse ethnic population to produce more accurate results.
Nursing research should also concentrate on the creation of specialised teaching methods that can be included into the undergraduate nursing curriculum to teach students about pain management in an efficient manner. This will surely give students the chance to treat cancer patients with chronic pain effectively and to encourage better patient outcomes in terms of pain management.
References
.png)
.png)

- Assignment - Child Care
- Assignment - Mathematics
- Assignment - Accounting
- Assignment - Auditing
- Assignment - Biology
- Assignment - Law
- Assignment - Management
- Assignment - Nursing
- Assignment - Finance
- Assignment - Computer Science and IT
- Assignment - Humanities
- Assignment - Economics
- Assignment - Statistics
- Assignment - Architecture
- Assignment - Engineering
- Assignment - cookery
- Assignment - Marketing
- Case Study - Chemistry
- Case Study - Accounting
- Case Study - Law
- Case Study - Management
- Case Study - Nursing
- Case Study - Finance
- Case Study - Computer Science and IT
- Case Study - Engineering
- Case Study - Economics
- Case Study - Biology
- Case Study - Auditing
- Case Study - Marketing
- Case Study - Project Management
- Coursework - Diploma
- Coursework - Accounting
- Coursework - Auditing
- Coursework - Biology
- Coursework - Management
- Coursework - Nursing
- Coursework - Finance
- Coursework - Computer Science and IT
- Coursework - Engineering
- Coursework - Humanities
- Coursework - Child Care
- Coursework - Project Management
- Coursework - Economics
- Coursework - Cookery
- Coursework - Law
- Dissertation - Accounting
- Dissertation - Auditing
- Dissertation - Biology
- Dissertation - Law
- Dissertation - Management
- Dissertation - Nursing
- Dissertation - Finance
- Dissertation - Computer Science and IT
- Dissertation - Humanities
- Dissertation - Economics
- Essay - Politics
- Essay - Childcare
- Essay - Accounting
- Essay - Biology
- Essay - Law
- Essay - Management
- Essay - Nursing
- Essay - Computer Science and IT
- Essay - Humanities
- Essay - Economics
- Essay - Auditing
- Essay - Engineering
- Essay - Architecture
- Essay - Finance
- Essay - Science
- Essay - Marketing
- Programming - Computer Science and IT
- Reports - Management
- Reports - Computer Science and IT
- Reports - Project Management
- Reports - Marketing
- Reports - Nursing
- Reports - Engineering
- Reports - Accounting
- Reports - Humanities
- Reports - Finance
- Reports - Architecture
- Reports - Biology
- Reports - Economics
- Reports - Childcare
- Reports - Law
- Research - Accounting
- Research - Auditing
- Research - Biology
- Research - Law
- Research - Management
- Research - Nursing
- Research - Finance
- Research - Computer Science and IT
- Research - Science
- Research - Engineering
- Research - Humanities
- Research - Economics
- Research - Project Management
- Research - Statistics
- Research - Architecture
- Research - Marketing
- Thesis Writing - Computer Science and IT
- Thesis Writing - Engineering
- Thesis Writing - Biology
- Thesis Writing - Finance
- Thesis Writing - Humanities
- Thesis Writing - Auditing
- Thesis Writing - Economics
- Thesis Writing - Law
- Thesis Writing - Nursing
- Thesis Writing - Accounting
- Thesis Writing - Architecture

.png)
~5.png)
.png)
~1.png)



















































.png)






