DEME20002 Supporting and caring for people with Dementia Assignment Sample
Learning Outcomes Assessed
1. Analyse the diverse presentations of people with dementia and the impact this may have on their care.
2. Demonstrate the comprehensive assessment of people at risk of or experiencing dementia.
Aim
The aim of this portfolio is for you to demonstrate your ability to appropriately assess the diverse presentations of people with dementia using a comprehensive assessment tool.
Instructions
There are three parts to this portfolio.
Part one: Select two case studies located on Moodle and describe the presentation of the two people with dementia.
Part two: Explain how diverse presentations of people with dementia may impact the care delivered to them by health professionals.
Part three: Describe and justify your comprehensive assessment of the people in the two case studies selected. This assessment must include physiological, psychosocial, and cognitive assessment.
Ensure each part of the e-portfolio is substantiated with peer-reviewed literature.
Literature and references
The number of references you should use is not limited. You should consider using references when you have used material from another source .You may also use seminal scholarly literature where relevant. Additional suitable references include textbooks and credible websites. When sourcing information, consider the 5 elements of a quality reference: currency, authority, relevance, objectivity, and coverage. Grey literature sourced from the internet must be from reputable websites such as from government, university, or peak national bodies: for example, the Australian College of Nursing.
Case study
Case Study 2. Mary Hobson.
Mary is a fifty-three-year-old woman who resides in the Fairfield Elsis Residential Aged Care Facility. She has lived in the facility for three years, after being found by neighbours in her house, on the ground, following a fall. Mary has no next of kin and her medical records indicate that she has previously had children, however, she does not appear to have contact with any of them at present. Mary needs encouragement with all areas of ADL care. She will commonly sit for hours on end unless she is encouraged to move. The facility has asked you to come in and assess Mary and suggest some strategies to motive and inspire her to increase her activity.
Meeting with Mary
When you meet with Mary, she immediately embraces you, and calls you the name of one of her children. She asks you about the football and grins widely as she talks happily of how Collingwood is likely to win the grand final. She talks about many different topics: cake making, cathedral windows, and sings hymns through your conversation. She seems very pleased that you have come to visit. She is less motivated to move from her
seat and when you suggest a walk, she says “No no no no...”. She looks slightly disturbed that you want her to move. You notice that toward the end of the meeting, she begins to become slightly over familiar, and you notice that there is a change in her demeanour.
Significant history
Mary has quite a lengthy medical history listed in her notes, involving injuries from previous falls (one only a few weeks ago), dental issues, bunions on both feet, arthritis in her legs and fingers, vitamin B deficiency, anorexia, previous diagnosis of alcoholism, and a past diagnosis of depression, along with her diagnosis of early-onset dementia, possibly alcohol-related dementia.
SOLUTION
Presentation of two people with dementia:
Mary (53 y, Female): The presentation of her symptoms of dementia indicates that she currently does not have any contact with any of her children, nor does she have any close relative to care for her. Her symptoms show that she has absolute disinterest to move, walk or be active.
In addition, she needs encouragement in all areas of daily-life activities. Also, the meeting with Mary has confirmed that she suffers from delusions and hallucinations because she was taking the names of her children and having some conversations about football matches, cathedral, and cake making that were not relevant indeed.
(Barry &75y, Male): Barry resides with his son at his residence who cares about his food and also gives him company. The case about Barry suggests that he has post-traumatic stress resulted from the Vietnam war. Barry has some frightening memories of the Vietnam war and thus suffers from panic attacks and sleep deprivation. Barry’s disease is called vascular dementia (Gowan & Roller, 2019). As suggested in the case study, Barry had recently suffered a stroke and that might have blocked an artery in the brain.
Part two
The way diverse presentations of dementia patients influence care delivery:
The diverse presentation of dementia affects the care delivery process because all patients have unique symptoms and have unique life experiences. In the case of Mary, she has no interest in moving or having doing activity. She suffers from delusions, hallucinations and many underlined diseases such as deficiency of Vitamin B, anorexia, dental issues, and many others. Her past medical history confirms that she has multiple issues and alcohol-related dementia. Patients like Mary need empathy because emotional support provides patience and insights to them. Thus, treating these patients with empathy would generate better care outcomes (Arvanitakis, Shah & Bennett, 2019).
However, in the case of Barry, he is suffering from post-traumatic stress disorder (PTSD) followed by the Vietnam war. He has traumatic memories of the war and gets panic attacks and sleepless nights. His condition reveals that he is not comfortable sharing much about the experience of the war. In addition, Barry also undergone a stroke which resulted in visio-perceptual difficulties. Since Barry is resistive in nature but is open to discussion for possibilities, an effective CBT would help him combat the issues.
Impact of the assessment on nursing care:
The care delivery process by nurses for dementia patients depends on their age, history of their life experiences, severity of dementia, and the presence of other underlying medical conditions (Kim, 2019). Referring to the case study of Mary, patients like her must be provided with suitable tools like an easy chair where they can feel comfortable. Also, ssome familiar and interesting decorations can make them feel engaged to their surroundings. These might encourage them to be more mobile and be active. Also, caregivers and nurses must empathize with patients like Mary and avoid questioning them (Harrison et al., 2018).
Furthermore, patients like Barry often need psychological therapeutic interventions. Gowan & Roller (2019) suggests that psychotherapies and Cognitive Behavioural Therapy can effectively help patients with vascular dementia and post-traumatic stress. For these patients, the nurses must also consider exposure treatments. Thus, it can be said that the diverse presentation of people with dementia tends to influence the way of care delivery by health professionals.
Part three
Comprehensive assessment for Mary:
Physiological: The falls risk assessment of Mary reveals she has high risk of falling as she was found collapsed on the floor before being admitted to the care unit. Also, she is immobile and has number of underlined diseases like anorexia, previous alcoholism, deficiency of Vitamin B and so on. Additionally, the pressure ulcer risks for Mary are also high as she was an alcohol and thus has high chances of liver ulcers. Moreover, the deficiency of Vitamin B can lead to mouth ulcers.
Psychological: Tools like Beck Depression Inventory (BDI) can be used to assess her depression and anxiety. Diagnosis reveals that she still longs for her children and is lonely. The psychological assessment reveals that refusal to walk or move can be characterized by old-age, increasing severity of dementia, orthopaedic aspects, and decreased functionalities. This assessment is important as this reveals about the psychological status of the patients and hence determines the care giving procedure.
Cognitive: The tools like Cognitive Impairment Scale PAS can be used for assessing her cognitive aspects. The diagnosis reveals that she was suffering from cognitive decline and having hallucinations and hence have been facing difficulties with her ADLs.
Comprehensive assessment for Barry:
Physiological: The falls risk assessment of Barry reveals that he has high risk of falling as he has visio-perceptual issues and depression. His old age can be another contributing reason to his falls risk. The pressure ulcer assessment of Barry’s case reveals that he does not have any symptom of developing ulcers and hence the risk is low. Barry must be exposed to some like-minded people as him with whom he can connect and communicate easily.
Psychological: The psychological assessment tool like Cognitive and neuropsychological tests can be used to determine his anxiety and depression scales (Beckman et al., 2019). The diagnosis reveals that barry has declining thinking skills and he finds it difficult to connect and communicate with people. This assessment would help the care givers to determine the level of care needed and to give the most suitable psychotic therapies.
Cognitive: The cognitive assessment can be done through Dementia Severity Rating Scale (DSRS). This assessment reveals that the type of dementia Barry has entails reasoning, memory, planning, and other types of thought processes resulted from the trauma of the Vietnam war. A recent psychological theory called Emotional Processing Theory states that the exposure treatments can be helpful for these patients’ cognitive condition as it would prevent the trauma memories to be negatively incorporated within their brain (Hayes, 2015).
References
Arvanitakis, Z., Shah, R. C., & Bennett, D. A. (2019). Diagnosis and management of dementia. Jama, 322(16), 1589-1599. https://jamanetwork.com/journals/jama/article-abstract/2753376
Beckman, E., Lazar, K., Van Hulle, C., Cole, A., Asthana, S., & Gleason, C. (2019). Association of traumatic brain injury, post-traumatic stress disorder and vascular risk with cognitive function in a veteran population: the brave study. Alzheimer's & Dementia, 15, P1559-P1559. https://doi.org/10.1016/j.jalz.2019.08.160
Gowan, J., & Roller, L. (2019). Changed behaviours in people with dementia. AJP: The Australian Journal of Pharmacy, 100(1180), 69–77. https://doi.10.3316/informit.320828203940274
Harrison, S., Cations, M., Jessop, T., Hilmer, S., Sawan, M., & Brodaty, H. (2018). Approaches to deprescribing psychotropic medications for changed behaviours in long-term care residents living with dementia. Drugs & Aging, 36(2), 125-136. https://doi.org/10.1007/s40266-018-0623-6
Hayes, A. (2015). Facilitating emotional processing in depression: the application of exposure principles. Current Opinion In Psychology, 4, 61-66. https://doi.org/10.1016/j.copsyc.2015.03.032
Kim, H. (2019). An analysis of the need for aid tools in dementia patients: focusing on the normal elderly, dementia patients, and caregivers of dementia patients. Indian Journal of Public Health Research & Development, 10(11), 4399. https://doi.org/10.5958/0976-5506.2019.04300.6
NURS3015 Health Variations 4 – Acute Life Threatening Condition
Case Analysis- Case Study of an Acute Life-Threatening Condition
Word Count
There is a word limit of 1000 words. Use your computer to total the number of words used in your assignment. However, do not include the reference list at the end of your assignment in the word count. In-text citations will be included in the additional 10%-word count. If you exceed the word count by 10% (1100 words) the marker will stop marking.
Aim of assessment
The aim of this assessment is to enable students to:
1. Demonstrate knowledge by analysing the information provided in the case study.
2. Apply the clinical information provided in the case study and describe this clinical information within a pathophysiological and patient focused framework.
3. Discuss nursing strategies and evidence-based rationales to manage a patient with acute heart failure
4. Discuss the pharmacological interventions related to the management of a patient with acute heart failure
Details
You are to answer all questions related to the case study provided for assignment help. Your answers must be directly related to the clinical manifestations that your patient presents with. You must submit your work with a minimum of six references from the past 5 years including peer-reviewed journal articles, textbook material or other appropriate evidence-based resources.
Case study
Mr. Aloha Das is a 68-year-old gentleman presenting to the emergency department at 0400hrs with worsening shortness of breath. Onset 2 days ago and progressively worsening. He also developed wheeze and right sided pleuritic chest pain this morning. Vomited x1, ongoing nausea. Has history of non-compliance with medication and adherence to fluid restriction.
Past History
Hypertension, Inferior Myocardial Infarction in 2020, Heart Failure, non-ischemic Cardiomyopathy, Permanent Pacemaker inserted 2021, DM Type II, GORD, Osteoarthritis.
Current medications:
Furosemide 40mg OD, Captopril 6.25 mg TiD, Digoxin 0.125 mg BD, Metformin 500mg TiD, Nexium 40 mg BD.
On 1.2 L fluid restriction; Echocardiogram results in 2021- systolic dysfunction, mild mitral valve regurgitation, dilated left atrium and ejection fraction (EF) 33%.
Plan
• Continuous cardiac monitoring
• 12 lead ECG
• Blood pathology order
• Troponin I High Sensitivity
• Chest X-Ray
• Insert IVC right hand
• Furosemide 40mg IV Stat
• Echocardiogram
Results of Investigations:
Chest x- ray: Left ventricular hypertrophy, interstitial edema noted by Kerley B lines in the costophrenic angle.
Blood Results:
Electrolyte, urea and creatinine:
Result/ Reference Range
Sodium - 137 mmol/L 135-147 mmol/L
Potassium - 3.9 mmol/L 3.5-5.2 mmol/L
Chloride- 105 mmol/L 95-107 mmol/L
Urea nitrogen(BUN) - 14.0 mmol/L 3.0-8.0 mmol/L
Creatinine- 147 μmol/L 64 -104 μmol/L
Question 1
In order to prioritise your nursing actions, you are expected to have a sound understanding of the pathogenesis and pathophysiology.
Explain the pathogenesis and pathophysiology causing the clinical manifestations with which Mr Das presents.
Question 2
Choose one high priority nursing intervention that you will perform for Mr Das
– Briefly explain why you chose this nursing intervention
– Explain how the nursing intervention will alleviate the clinical features of Mr Das using physiological linking
– Describe briefly the impact of not performing the intervention
Question 3
Mr Das has been prescribed Furosemide 40mg IV Stat and Glyceryl Trinitrate IV Infusion 10 mcg/min starting rate.
For both medications explain
– The mechanism of action
– Why your patient is receiving this medication in relation to his symptoms and diagnosis?
– What are the nursing considerations for this medication?
– What clinical response you expect?
– What continuing clinical observations will you need to undertake?
Submission
Refer to Section 2.5 of the Learning Guide- General Submission Requirements Submit your assessment through Turnitin
Format
All assignments are to be typed Typing must be according to the following format:
3 cm left and right margins, double spaced.
Font: Arial or Times New Roman
Font size: 12pt
See further submission requirements below
Submission Requirements
1. Electronic copy only. Students are to submit an electronic copy of the assessment. Students are not required to submit the original hard copy of their assessment on campus
2. Submit your assessment electronically through the Turnitin link on the unit vUWS site.
3. Students are to upload the assessment with the following title: Surname_Firstname_assessment title
4. Your assessment must be submitted in .doc, docx format.
5. This assessment is marked online; no paper copy will be accepted. Marks, comments and the marking criteria will be released online. If you do not receive your marked assessment when all others have been returned, it is your responsibility to contact the Unit Coordinator for assistance.
Solution
Question 1:
RHD (Rheumatic heart disease) indicates a major cause of cardiovascular diseases. In this case study, a brief explanation of pathophysiology and pathogenesis causing the clinical manifestations with Mr. Das. This particular case study is based on the diagnosis and clinical manifestations of RHD for Mr. Das, and this includes pathogenesis, diagnosis, epidemiology, prevention of acute rheumatic, and treatment. According to this case study, a 68 years old gentleman, Mr. Das, presented himself to the emergency department with the condition of shortness of breath. It is seen that, 2 days ago, with progressive worsening, Mr. Das suffered and presented to the department of emergency at 0400 hrs.
Due to this, pathophysiology and pathogenesis caused clinical manifestations, and Mr. Das developed right side chest pain this morning along with on-going nausea and one-time vomiting. As per the case analysis of "Acute Life-Threatening Condition", this cannot be managed with successful results, and that is critically dependent on prompt therapy and early recognition (Caraher et al., 2018). For example, in the case of an "Acute Life-Threatening Condition", the person can face different symptoms before the death, and all the symptoms occur within 2-5 days after facing the first symptom.
Question 2:
A chosen high priority nursing intervention is “monitoring of vital signs and recovery progress” and that is considered as independent nursing intervention for this particular case study. Vital signs are most important component for this case of Mr. Das to monitor patient’s health as well as allow prompt detection for delaying recovery or addressing the breathing problem. Furthermore, several plans like Continuous cardiac monitoring, 12 lead ECG, Blood pathology order, Troponin I High Sensitivity, Chest x-ray, IVC insertion in right hand Furosemide 40mg IV Stat and Echocardiogram are included in the nursing intervention (Burchum & Rosenthal, 2021). Current medications include several medicines which are allocated for the patient where Furosemide 40mg OD, Captopril 6.25 mg TiD, Digoxin 0.125 mg BD, Metformin 500mg TiD, Nexium 40 mg BD are used.
On the other hand, on 1.2 L fluid restriction, Echocardiogram resulted in 2021- systolic dysfunction, mild mitral valve regurgitation, dilated left atrium and ejection fraction (EF) 33% are also utilised ((Lewis et al., 2020)). In the nursing assessment, several details of the patients have been discussed. Thus, “monitoring of vital signs and recovery progress” is best nursing intervention for this particular case of managing the health condition for Mr. Das.
Discussion of how a nursing intervention will alleviate the clinical features of Mr. Das physiological linking
As per the case study, a Nursing intervention will help to give alleviation to the patient, Mr. Das. After that, corresponding to the current medications as different medicines including Furosemide 40 mg OD, Captopril 6.25 mg TiD, Digoxin 0.125 mg BD, Metformin 500mg TiD, Nexium 40 mg BD have been allocated. Furosemide 40 mg OD is mainly used for the treatment of fluid retention blended with heart failure, including left ventricular failure. Besides, Captopril 6.25 mg TiD is used for congestive heart failure (Bullock et al., 2017). In order to treat irregular heartbeats, Digoxin 0.125 mg BD is used for the treatment of DM type 2 as Mr. Das is suffering from DM type 2 as per the case study. Creatinine and Urea nitrogen (BUN) is high from the reference rate. Along with that, Nexium 40 mg BD is utilised for the treatment of erosive reflux esophagitis, including the prevention of rebreeding of peptic ulcers. With several intervention reports like blood reports, x-ray and others report the right diagnosis will be taken as per the case study (Suen et al., 2020).
Describe the impact of not performing the intervention
In such accordance with not managing and performing a well nursing intervention, different issues can occur if the intervention is not performed as several medicines as per the case study is too significant for the treatment of heart failure and DM type 2 (Xu et al., 2018). If the restrictions cannot be performed, Mr. Das may suffer from several symptoms. Along with that, if blood reports and x-ray are not considered, medication will not be procured.
Question 3:
The mechanism of action
According to this case study, Mr. Das has been prescribed two medicines for his "Acute Life-Threatening Condition", and these are Furosemide 40 mg IV stat and Glyceryl Trinitrate IV Infusion 10 mcg/min in starting rate. For Mr. Das, the initial dose is to be administered through an intravenous application with 40 mg Furosemide, and if needed, another injection could have to be given after 30-60 minutes (Huether & McCance, 2019). On the other hand, according to the health condition of Mr. Das, Glyceryl Trinitrate IV Infusion 10 mcg/min has been given, and the dosage of 10 mcg/ min was able to obtain Glyceryl Trinitrate 6 ml of admixture/hour. These two prescribed medicines were helpful to manage his health condition at the starting rate.
Why is your patient receiving this medication to his diagnosis and symptoms?
In case of patient diagnosis and symptoms, Furosemide 40 mg IV stat helps the body get rid of some extra water by increasing the urine in the patient's body. Additionally, another one helps to reduce the tone of "vascular smooth muscle" (Atherton et al., 2018). After that, the action is more suitable to manage venous capacitance vessels compared to arterial vessels.
What are the nursing considerations for this medication?
Medication administration is a nursing intervention, and that includes five major activities for prescribing and managing the health of Mr. Das. These are such as diagnosis, implementation, assessment, planning, and evaluation.
What clinical response do you expect?
The major aim of the clinical response is to evaluate changes in lung volumes, diagnosis, and perception of breathing discomfort intensity with pharmacological intervention.
What continuing clinical observations will you need to undertake?
The major clinical observations in the case of "Acute Life-Threatening Condition" for Mr. Das is to manage the pathogenesis and pathophysiology causing the clinical manifestations along with ECG report, and checking irregular heartbeat and sugar test for DM type 2, and many more.
Reference
Atherton, J. J., Sindone, A., De Pasquale, C. G., Driscoll, A., MacDonald, P. S., Hopper, I., ... & Connell, C. (2018). National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: guidelines for the prevention, detection, and management of heart failure in Australia 2018. Heart, Lung and Circulation, 27(10), 1123-1208.https://www.heartlungcirc.org/article/S1443-9506(18)31777-3/fulltext
Burchum, J., & Rosenthal, L. (2021). Lehne's Pharmacology for Nursing Care E-Book. Elsevier Health Sciences.https://books.google.com/books?hl=en&lr=&id=VGNCEAAAQBAJ&oi=fnd&pg=PP1&dq=PHARMACOLOGY+NURSING+CARE++BOOK+Lehne%27s+pharmacology+for++nursing+care&ots=rRXRiaAdxd&sig=zF4O9V3tIDIScLRzMNYRkvNSLjI
Byrne, J. E., Bullock, B., & Murray, G. (2017). Development of a measure of sleep, circadian rhythms, and mood: the SCRAM questionnaire. Frontiers in psychology, 8, 2105. https://www.frontiersin.org/articles/10.3389/fpsyg.2017.02105/full
Caraher, M.C., Sophocleous, A., Beattie, J.R., O'Driscoll, O., Cummins, N.M., Brennan, O., O'Brien, F.J., Ralston, S.H., Bell, S.E., Towler, M. & Idris, A.I., (2018). Raman spectroscopy predicts the link between claw keratin and bone collagen structure in a rodent model of oestrogen deficiency. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1864(2), pp.398-406. https://www.sciencedirect.com/science/article/pii/S0925443917303848
Huether, S. E., & McCance, K. L. (2019). Understanding Pathophysiology-E-Book. Elsevier Health Sciences.http://repository.stikesrspadgs.ac.id/104/1/Study%20Guide%20for%20Understanding%20Pathophysiology-345hlm.pdf
Lewis, P., Wilson, N. J., Hunt, L., & Whitehead, L. (2020). 1 Nursing in Australia. Nursing in Australia: Contemporary Professional and Practice Insights.https://api.taylorfrancis.com/content/books/mono/download?identifierName=doi&identifierValue=10.4324/9781003120698&type=googlepdf
Suen, L. K. P., Guo, Y. P., Ho, S. S. K., Au-Yeung, C. H., & Lam, S. C. (2020). Comparing mask fit and usability of traditional and nanofibre N95 filtering facepiece respirators before and after nursing procedures. Journal of Hospital Infection, 104(3), 336-343. https://www.karger.com/Article/PDF/488001
Xu, S., Zhang, Z., Wang, A., Zhu, J., Tang, H., & Zhu, X. (2018). Effect of self-efficacy intervention on quality of life of patients with intestinal stoma. Gastroenterology Nursing, 41(4), 341. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6078485/
PBHL20010 Case study Assignment Sample
The first assessment task is a case study of about 2000 words that you will complete on an individual basis.
The case study will require you to choose one of the eight stakeholder groups listed below and discuss their role in a public health emergency; the nature and direction of their interest based on their position in the community and their function in society; and the factors that may affect their actions. You must also choose a specific emergency situation from which you will draw examples to illustrate your discussion. This may be an epidemic of disease (for example, the COVID19 pandemic); a natural disaster (flood, bushfire, earthquake, etc); or an anthropogenic event (chemical spill, industrial explosion, etc). You ust specific the emergency and stakeholder groups clearly in the introduction to the case study. You will also need to use appropriate academic references to support your understanding of stakeholder participation, communication needs, responsibilities, and so forth as relevant.
The stakeholders you may choose from are:
1. Local government
2. Science/health experts
3. Local business interests
4. The media
5. Representatives of the long-term community (people who have lived in a given location for 10 years or more)
6. Representatives of new groups (people who have recently arrived in or moved to a given location)
7. Local health care personnel
8. State (or higher level) government
Your case study must have the following sections for assignment help
1) Introduction – identifies the chosen stakeholder, the emergency and gives a general indication of who they are or what they do;
2) Roles in a Public health Event – for the stakeholder group you have chosen, describe their role in a public health emergency; make sure to consider whether their role is official or non-official and whether they are personally at risk of health impacts and the other kinds of risk they experience;
3) Risks and Responsibilities – for the group you have chosen, describe the nature of the risks identified in the previous section; make sure to consider whether the risk is direct or indirect, whether it is a risk to health or another kind of risk, what the specific health or non-health risk involves, and what the group’s responsibilities are in relation to the public health emergency and its own and the risks of other stakeholders;
4) Role in Public health Decision-Making – for the group you have chosen, consider how they contribute to decision-making in the context of a public health emergency; be sure to discuss whether their contribution is official or unofficial, the channel through which they might affect the decision-making process. and the degree to which their impact is informed by evidence-based and non-evidence-based knowledge; and
5) Conclusion – discuss the position of the stakeholder group you have chosen in a public health emergency; you may want to consider whether they are actors or bystanders, for example, or use some other classification, but be sure to state whether your chosen stakeholder group is likely to be affected significantly, the nature of the impact, and why you believe this would occur. This assignment must be written in a formal, academic style (not first person) and must be fully referenced. Harvard referencing is preferred for this unit. If you need help with referencing, please consult the referencing guides available online and through the Library as soon as possible.
Solution
Introduction
In this paper, a discussion regarding the role of a particular stakeholder group in regard to a public health emergency is going to be elaborated. The stakeholder group that has been chosen in order to make the discussion is the media, and the public health emergency that has been considered in this regard is Covid19. It can be regarded as the most considerable public health emergency in the current situation. The emergency has caused a significant number of deaths throughout the world, and it has caused harm to public health considerably. Along with providing a significant effect on public health, it has caused economic shock to a number of countries. However, the matter is that the media was supposed to play a vital role in regard to the process of making people aware of the emergency and the situational needs, and by considering this key area, the overall discussion is going to be elaborated on here.
Roles in a public health event
Roles
Covid19 is a global infectious disease that emerged from Wuhan, Chin (Anwar et al., 2020). The media can be regarded as the main mean of mass communication that includes radio, television, the internet, newspapers and others. People who are associated with media are mainly responsible to make people aware of the current situation based on every aspect related to society, politics, economic factor, technical area, environmental hazards, health situations, and others. It means that in regard to such a situation where a pandemic has been spreading in an effective manner and causing numerous deaths and affecting uncountable number of people, they were supposed to play an important role in making people aware of the situation. In this regard, their roles have been as follows:
Making people aware of the situation
It can be regarded as the key role of the chosen stakeholder group with respect to the concerned emergency situation. They have been supposed to make people aware of every day’s update, such as the death rates related to Covid19, the way the infection has been spreading each day, what is the current situation of the local area and the world as well. They have been supposed to make people understand the severity of the issue by letting them know about these factors. At the time when people become aware of the severity of a situation, they are able to make the right decision based on the situational needs, and that is why the media has been responsible to make them aware of the situational needs so that they can manipulate their lifestyle and become interested in living a restricted life by considering the emergency of the situation.
Providing authentic information regarding the emergency of the situation
The media, in regard to the situation of a healthcare emergency is responsible to provide authentic information to people so that they can understand the actual scenario and make decision properly based on it. By considering the viewpoint of Mheidlyand Fares (2020), it can be stated that media is a powerful avenue for the dissemination of wellness education. In regard to Covid19, the media was responsible to do the same, From death rates to infection spreading rates, everything are required to be communicated with people while maintaining the highest level of authenticity so that they can understand what they should do in a particular situation in order to be safe. In this case, the media is not likely to be influenced by any political influences. They have been responsible to maintain authenticity with respect to each word they have been sharing with people as the situation has been complex and crucial. Any misleading word of the media might lead people improperly and it would enhance the severity of the issue.
Leading people to the right path in crucial moments
People have been panicked in the situation with the increasing number of deaths and infection rates. At that time period, it has been the responsibility of the media to understand how they should live their lives in order to keep themselves and their family members safe. Instead of making people scared, they have been supposed to encourage them to maintain all safety and precautionary measures so that the situation can be controlled properly.
Whether the role is official or non-official
The roles of the media that have been highlighted in the above-stated passages are definitely official. At the time of public crisis, media is required to ensure to communicate crisis information effectively (Latifet al., 2020). By considering the official responsibilities of media, it can be stated that they are professionally responsible to gather and update information regarding any situation, and correct information throughout the life of a news story. They are also professionally responsible to provide facts that can allow people to be better informed about any issue that matters to the society and the lives of people. It means that covering the Covid-19-based issues can be regarded as the key responsibility of these people and it can also been stated that by considering the official terms and conditions, that these people have to follow, it has been their official responsibility to make people aware of the situational needs, the emergency of the situation, and the way to control the situation. They have been supposed to work by considering that if they can make people aware of these facts and if they can reach people properly, controlling the situation would be easier and battling with the health emergency would also be easier. Hence, it can be concluded that all of the responsibilities highlighted above can be regarded as the official responsibility of these people and they have been supposed to handle these responsibilities by considering the professional ethics of them.
Their personal risk
In this situation, they have some personal risks, and these are mainly about their health. Throughout 2020- 2021 and the beginning of 2022, the spreading rates of Covid-19 were considerable.
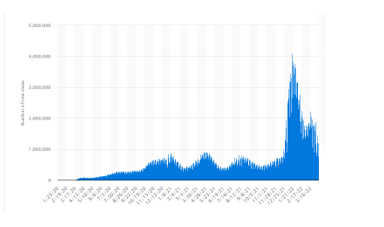
Figure 1: Covid19 spreading rates
(Source: Statista, 2022)
The graph is showing the same. In such a situation working with public was a considerable risk for the media as they could be affected anytime as they did not have any scope to isolate themselves from people who were affected. It can be regarded as a major health concern that these people have faced in this situation. In the following section, a detailed discussion regarding the risks is going to be elaborated on.
Risks and responsibilities
Nature of the risk
In the above-stated passages, the risk has been identified, and when the matter comes to making a discussion regarding the nature of the risk it has to be stated that the risk was supposed to impact the stakeholders directly, and it can also be stated that the risk was mainly related to the health of these people and the family members of them. Covid19 is a significant global and public health crisis (Banerjee and Rao, 2020). These stakeholders were supposed to meet with public by considering their professional roles and responsibilities, and that is why they were supposed to be infected in the fastest manner. In this regard, it is also important to state that they have not been free from the risk yet as Covid-19 is still causing harms and death though the infection rates have been decreased, and it means that these people are still dealing with such risks.
Another important risk to be considered here is about their economic and professional security. By considering the information shared by Radcliffe(2020), it can be stated that a number of people have lost their jobs in the Covid19 phase as a number of news companies have been laid off in the Covid19 phase. This situation has actually affected their professional and economic security of these people. It can be regarded as a direct risk to be considered here as it has directly impacted the overall lifestyles of these people in a devastating manner.
Responsibilities of the group in public health emergency
From professional aspect, they are responsible to collect information regarding the current status of Covid19 and it has been the responsibility of them to provide people with accurate information so that they can understand the situational needs and they can take steps based on the same. It has been their responsibility to make people aware of the precautionary measures so that they can deal with the situation perfectly. They have been supposed to provide information not only regarding the impact of the issue on public health but also the impact of the issue on political and economic aspects. In order to avoid risk of Covid-19, effective government interventions have been implemented, and it has been the responsibility of media people to make individuals know about these (Liu et al., 2021). They have been responsible to ensure that people understand the situational needs properly and make decisions based on it.
The risks of other stakeholders
In this regard, other stakeholders were also supposed to face some issues. Along with journalists, press and camera man, some other people work with media people and that includes the drivers of the vehicle that these people are using, their assistants, and others, and these people are supposed to be infected if these people get infected. It means that with the risk of the chosen stakeholders, the risks of other stakeholders are interrelated.
Role in public decision making process
How they contribute to decision making
Bridgmanet al.,(2020) have stated that if people spend time in media that provide misinformation, they are likely to develop wrong attitudes and behaviors. These people are responsible to provide a significant impact on public decision making process. They have been responsible to make people aware of Covid-19 situation that can influence the decision-making process of them. They have been responsible to make people understand the precautionary measures instead of causing them to get panicked. They have been responsible to maintain the highest level of integrity and honesty in regard to the data collection and communication process so that any individual would not be misled and they van make the best decision by considering the actual situational perspectives.
Whether the contribution is official or unofficial
By considering professional aspect, it can be stated that media people are supposed to make people aware of a situation and his kind of awareness can influence the decision-making process of individuals in a considerable manner. From this perspective, it can be stated that the contribution of them that has been highlighted in the above-stated passages is completely official.
The channel through which they can affect the decision-making process
Media people can be associated with any channel that includes newspapers, television, internet and others. From this perspective, it can be stated that all of these channels can be used in order to affect the decision-making process of people. In other words, it can be stated that media people are sharing information by using all of these channels and this information is effective enough to influence the decision-0making process of people, and that is why it can be stated that newspaper, television, radio, and the internet are some channels through which media people can influence the decision-making process of people.
The degree with respect to their impact in this regard
In the above-stated passages, a discussion regarding the way they can influence the decision-making process of people has been elaborated, and by considering the same, it can be stated that the degree to which they can impact the decision-making process is high as they are the primary resource of information for mass people. By considering their viewpoint, mass people have been judging the Covid-19 situation and the way they have to deal; with it. Hence, the degree with respect to their impact in regard to the decision-making process is high.
Conclusion
In the above-stated passage, a detailed discussion regarding the impact of the media on a health emergency (Covid-19) has been elaborated. By considering the discussion, it can be stated that these people have been playing a vital role in the context while providing people with authentic information and making them aware of the situation. They have been contributing to the decision-making process of people in an effective manner as per their professional responsibilities while dealing with considerable risks. By considering the way the stakeholders are playing the role of actors with respect to the situation. Based on the actions of them, the way people can think and manage the issue is being changed, and it means that they are playing the role of actors in this regard. The situation can impacted their lives effectively as it has already been stated that they have been dealing with considerable health risks. Apart from that, they were dealing with job security-layered issues. Health risks can impacted their action with respect to the situational needs and it could prevent them from following their roles and responsibilities. On the other hand, job security issues associated with the situation could affect them physical and mental well-being. The situation-related discussion has been made, and based on the situational perspective, it has been possible to understand that such issues could occur.
References
Anwar, A., Malik, M., Raees, V. and Anwar, A., 2020.Role of mass media and public health communications in the COVID-19 pandemic. Cureus, 12(9).https://www.cureus.com/articles/38293-role-of-mass-media-and-public-health-communications-in-the-covid-19-pandemic
Banerjee, D. and Rao, T.S., 2020. Psychology of misinformation and the media: Insights from the COVID-19 pandemic. Indian Journal of Social Psychiatry, 36(5), p.131.
Bridgman, A., Merkley, E., Loewen, P.J., Owen, T., Ruths, D., Teichmann, L. and Zhilin, O., 2020. The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. Harvard Kennedy School Misinformation Review, 1(3).https://www.indjsp.org/article.asp?issn=0971-9962;year=2020;volume=36;issue=5;spage=131;epage=137;aulast=Banerjee
Latif, F., Bashir, M.F., Komal, B. and Tan, D., 2020.Role of electronic media in mitigating the psychological impacts of novel coronavirus (COVID-19). Psychiatry research, 289, p.113041.https://www.sciencedirect.com/science/article/pii/S0165178120309380
Liu, N., Chen, Z. and Bao, G., 2021. Role of media coverage in mitigating COVID-19 transmission: Evidence from China. Technological Forecasting and Social Change, 163, p.120435.https://www.sciencedirect.com/science/article/pii/S0040162520312610
Mheidly, N. and Fares, J., 2020.Leveraging media and health communication strategies to overcome the COVID-19 infodemic. Journal of public health policy, 41(4), pp.410-420.https://link.springer.com/article/10.1057/s41271-020-00247-w
Radcliffe, D., 2020. Covid-19 has ravaged American newsrooms–here’s why that matters. Available at SSRN 3693903.https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3693903
Statista, 2022. COVID-19 new cases worldwide by day | Statista. [online] Statista. Available at: <https://www.statista.com/statistics/1103046/new-coronavirus-covid19-cases-number-worldwide-by-day/> [Accessed 18 April 2022].
NURS3002 Advance Decision Making and Practice Assignment Sample
Length: 1500 words
Curriculum Mode:
There is a word limit of 1500 words. Use your computer to total the number of words used in your assignment. However, At not include the reference list at the end of your assignment in the word count. In-text citations will be included in the additional 10% word count. If you exceed the word limit by more than 10% the marker will stop marking at 1500 words plus 10%.
Aim of Assessment:
The Aim of this assessment is to develop your understanding evaluating the professional conduct of a nurse/midwife in the case study provided.
The case study provided is a decision statement selected from Decisions of the Professional Standards Committee from the Nursing and Midwifery Council New South Wales - The Health Care Complains Commission (HCCC). You are to identify professional practice issues from the case study and then draw on the professional frameworks and regulatory legislation, to develop sound and appropriate responses to the clinical incident that will inform your future practice.
Details for Assignment Help
This assessment requires you to identify and summarise the professional practice issues in the case study from either a nursing or midwifery practice perspective. You need to identify and evaluate relevant professional errors identified that potentially contributed to the incident happening. Finally, discuss on how your future practice might change and develop as a result of this learning.
Students are to draw on the National Safety and Quality Health Service (NSQHS) Standards, NMBA professional practice documents and NSW Health policy documents (where appropriate) to develop informed responses.
Students must refer to and use the case studies located on vUWS under Assessment 2 tab for this assessment. There is one nursing case study and one midwifery case study to choose from. Submission requirements: -
The total word count is 1500 words. - Electronic copy only.
- This assessment is marked online; no paper copy will be accepted. Marks, comments, and the marking criteria will be released online. If you do not receive your marked assessment when all others have been returned, it is your responsibility to contact the Subject Coordinators for assistance.
Solution
Introduction
The professional code of conduct of a nurse embodies an ethical blend of rules and norms that is designed to direct the nurse in providing care to the patients found in critical care situations. The code of ethics comprises veneration for beneficence, autonomy, non-maleficence and justice. The essay consists of three sections. The first section discusses the professional practice issues from the perspective of a nurse. The second section points out the relevant professional errors of two nurses from the case study. In addition, the NSW Health policy documents mark the guidelines to be followed by the nurses rendering service to critical care patients. Finally, the third section discusses the reflection on how the suggested practices might amend and mitigate the issues found in the incident of the case study. The essay identifies the relevant professional errors from the case study and shows that the professional code of conduct followed by the nurses can help to resolve issues.
Section 1
The incident in the case study points out the complaint that has been launched against Ms Nelly Youssef who is a registered nurse. The complaint was launched against Ms Nelley Youssef by the Health Care Complaints Commission before the Administrative Tribunal and NSW Civil.
This complaint was lodged after an inspection of all the allegations charged against her on 13th January 2021 (Gillespie & Reader, 2018). All the allegations were proven, and she was charged with professional misconduct and unsatisfactory professional conduct. The case was filed against her after the Commission noticed an unprofessional act. They alleged her after they found an 80 year patient with a laryngeal stoma unresponsive. Ms Nelley Youssef reluctantly agreed with the junior colleague to dress the stoma and provided the dressing to the patients without proper instruction (Joo & Liu, 2021). Later, the patient was found not responding, thus it was tough for her to remove the dressing. When asked, she provided wrong information stating that she noticed the patient was not responding and the stoma was not covered. When found that the information provided was irrelevant, it was decided that strict actions would be taken against her. She misled her junior colleague (Gillespie & Reader, 2018).
Section 2
The incidents in the case study point out two professional errors committed by two nurses, Ms Nelley Youssef and RN Mc Arthur. Nelly Youssef was accused of unsatisfactory professional misconduct as she improperly responded to a request from a junior colleague who sought advice from her (Caselaw.nsw.gov, 2022). The former stated that it will cause no harm if Meplix occlusive dressing to the stoma of Patient A. By this, she portrayed inadequate knowledge that stoma is the only airway of patient A, covering which will lead to more harm than good. Moreover, the dressing was forgotten to be removed from the patient until he was found unresponsive in the shower. When she was accused of unprofessional conduct under 139B(1), she said she did not find Mepilex border dressing on the stoma. However, later on, she admitted that she lacked knowledge regarding Patient A's anatomy (Caselaw.nsw.gov, 2022). Moreover, she stated that she did not know that the laryngeal stoma was the only airway for the patient.
RN McArthur was also accused of the unprofessional code of conduct under 139B(1)(a). The concerned person also improperly applied a Meplix dressing on the patient's laryngeal stoma before he started to take his shower. Moreover, he also lacked adequate knowledge about the clinical history of the patient (Halcombet al. 2020). He also failed to know that the only airway of the patient is the laryngeal stoma which was unknowingly covered. He further stated that she stayed with the patient for five minutes after applying the dressing. This was falsely stated by the person in a letter sent to HCCC. He had further satiated that at the time of dressing he lacked the information about the underlying anatomy of patient A (Caselaw.nsw.gov, 2022). To everyone's utter surprise, he denies is not guilty of whatever has happened with the patient.
NSW health organisations monitor the incorporation of Policy Documents and guide the implementation as an essential aspect of strong governance, audit formulation and performance. The policy document consists of guidelines, policy directives and information issued by the NSW Ministry (NSWhealth, 2022). Besides encompassing protocols and procedures, it also lays down guidelines that should be strictly adhered to by the health service unit within the local health district. The policy documents formulate superior clinical practices along with the clinical and non-clinical functions. The guidelines are issued by the NSW policy systems and adopted in the NW health units. The components of the policy document are the information bulletin, NSW health organisation and the NSW ministry of health (NSWhealth, 2022). The policy document clearly explains the information bulletin, policy directive and essential guidelines issued by the NSW health organisation.
The organisation found in the case study does not follow the guidelines laid down by the National Safety and Quality in Health Service Standards (NSQSH). So, the company can opt for Safety and quality systems with the help of governance processes so that they can improve and manage the safety and quality of health care for patients (Australian Commission on Safety and Quality in Health Care, 2021). In addition, the NMBA guidelines are not ingrained in the mentioned health care unit of the case study. The NMBA states that nurses shall adhere to professional commitment and abide by the respective law (NMBA, 2022). Thus, the nurses are expected to act with professional obligation for the sake of the patient's recovery and well-being. As a result, the convicted nurses are placed under S139B (1) for conducting unprofessional behaviour (NSWhealth, 2022). The Health Care Complaints Commission (HCCC) has done justice to the complainant by identifying the accused and taking legal measures.
The implementation of the NSW policy documents gives an overview of the roles and responsibilities to incorporate the policy directives (Taylor et al. 2020). The policy documents comprise the codes of conduct that medical professionals are expected to follow. It provides a framework of actions with respect to ethical conduct. Breaching the code of conduct mentioned in the policy documents will be held responsible by law (NSWhealth, 2022). In addition, it leads to disciplinary actions and the punishment is decided by the severity of the crime.
Section 3
Reflection
I have been through both the cases and understood that the first case was related to Ms Nelley Youssef, against whom a case was filed due to her unprofessional negligence towards the dressing of stoma for an 80-year-old patient who was found not responding. At the same time, the second case deals with two professional misconducts by Ms Nelley Youssef and RN McArthur for reluctantly applying Meplix dressing to a patient with a laryngeal stoma (NMBA.gov., 2022). All I understand is that both cases are completely careless, or the nurses are not being provided with proper training. As per my understanding, an individual might own a degree and be an official nurse, but they can still be expected to make mistakes. In both cases, the situation could have been controlled if the nurse had asked for help from their other senior colleagues before conducting the method on the patients (Taylor et al. 2020). Both the patients have been found to act unprofessionally, first for misguiding their junior colleagues and second for showing a lack of adequate knowledge.
After summarising the cases, I had been through the NMBA Standards for Practice documents for Nurse and NSQHS or National Safety and Quality Health Service. I learnt about the patients' professional expectations and the nurse's authority. I can conclude that if I had been in place of Ms Nelley Youssef, I should have taken the responsibility and correctly instructed my junior colleague for the dressing of the laryngeal stoma firstly because the patient had not been responding and second because it was 80 years of age. This is not only the main reason but the main because, as a senior nurse, it is my responsibility to take care of the patients and properly guide the juniors (NMBA.gov., 2022). Thus, this would not have led me to any problems like Ms Nelley Youssef had. As per the case of RN McArthur, firstly, I would have strictly followed NMBA and NSQHS and still, if I was unclear about the procedures, I would have consulted someone, maybe a doctor or an experienced nurse. I would not have reluctantly applied Meplix on the patient's stoma before their bath. It is very unprofessional and showcases carelessness to state a lack of adequate knowledge about the wound (NMBA.gov., 2022). Even if that had happened, I would not have just strongly accepted that it was not my fault, even after knowing it was.
Conclusion
This study is concerned with summarising a case study that had been provided related to the issue or complaints that had been launched against the nurses for misleading or misconducting and performing unprofessional techniques of giving medication to the patients. Here the summary has been provided of the patient's complaints. The study has been divided into an introduction to the nursing case study talking about the professional code of conduct in nursing. Sections 1, 2, and 3 highlights the issues and summarise what the problems had been, under what act they have been taken, and what accusation points have been pointed at the nurses and how they had reacted to it. Reflection is the place where the cases have been heightened with the problems that the patients have faced due to the unprofessional acts of the nurses.
References
Australian Commission on Safety and Quality in Health Care (2021). National safety and quality in health service standards (2nd ed.). Retrieved 27th August 2022, from https://www.safetyandquality.gov.au/sites/default/files/2021-05/national_safety_and_quality_health_service_nsqhs_standards_second_edition_-_updated_may_2021.pdf.
Gillespie, A., & Reader, T. W. (2018). Patient?centered insights: using health care complaints to reveal hot spots and blind spots in quality and safety. The Milbank Quarterly, 96(3), 530-567. https://onlinelibrary.wiley.com/doi/pdfdirect/10.1111/1468-0009.12338
Halcomb, E., Williams, A., Ashley, C., McInnes, S., Stephen, C., Calma, K., & James, S. (2020). The support needs of Australian primary health care nurses during the COVID?19 pandemic. Journal of nursing management, 28(7), 1553-1560. https://doi.org/10.1101/2020.06.19.20135996
HCCC v Youssef & McArthur [2021] NSWCATOD 2
Health Care Complaints Commission v Youssef; Health Care Complaints Commission v McArthur - NSW Caselaw. Caselaw.nsw.gov.au. (2022). Retrieved 27th August 2022, from https://www.caselaw.nsw.gov.au/decision/176ee7c5bee2c2cdb86225c8.
Joo, J. Y., & Liu, M. F. (2021). Nurses' barriers to caring for patients with COVID?19: a qualitative systematic review. International nursing review, 68(2), 202-213. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8013562/
NMBA.gov. (2022). Retrieved 29th August 2022, from https://www.nursingmidwiferyboard.gov.au/codes-guidelines-statements/professional-standards/registered-nurse-standards-for-practice.aspx
Taylor, E. V., Lyford, M., Parsons, L., Mason, T., Sabesan, S., & Thompson, S. C. (2020). "We're very much part of the team here": A culture of respect for Indigenous health workforce transforms Indigenous health care. PLoS One, 15(9), e0239207. https://doi.org/10.1371/journal.pone.0239207
Www1.health.nsw.gov.au. (2022). Retrieved 27th August 2022, from https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2016_049.pdf.
HAS108 Health Assessment Sample
Individual/Group Individual
Length 2000 words (+/- 10%)
Learning Outcomes
The Subject Learning Outcomes demonstrated by successful completion of the task below include:
b) Identify and demonstrate interview techniques used to enhance communication during history taking
c) Discuss ways to incorporate health teaching as part of the health assessment
d) Perform a thorough and accurate holistic health assessment
e) Discuss the importance of understanding the diversity of society and cultural safety approaches that influences the approach to healthcare
f) Recognise elements of the development of person centred care plans
This assessment requires you to answer 3 questions. The questions are the same for each character however, given the different circumstances, socio-economic and medical histories of the characters, each case study is to be uniquely considered.
Short Answer Questions for case study assignment help -
1) Using resources provided in this subject, identify and explain what information is needed to a gain a more comprehensive past history for your chosen video character. Consider the patients level of health literacy and cultural safety issues in your answer.
2) Based on the information given for each character, identify and explain what abnormalities/concerns you can identify in the physical observations and patient history.
3) Identify and explain what additional physical assessments are needed in order to facilitate a diagnosis for your chosen character, and identify and describe what body systems need to be explored further.
Theo
PULSE: 70 bpm (resting), 100 bpm (on exertion).
TEMPERATURE: 37.5 ?C
RESPIRATION: 18 (Theo reports thick secretions, ‘worse when getting up in the morning’, primary auscultation- audible moist cough that Theo states ‘is hard to get rid of’).
SaO2: 95% room air (RA)
WEIGHT: Body Mass Index (BMI) 16.
BP: 100/70 mmHg
CNS: GCS 15
GENERAL APPEARANCE: Dishevelled, tooth decay, nicotine stained fingers, initial visual inspection
Theo observed to have to have minimal body fat.
Mobility: ambulant does not appear to have any deficits.
Urinalysis: Leukocytes ++. Slight Specific Gravity increase of 1.010.
Solution
1. Title and a brief summary
Personal Improvement Plan
From this project, it can be understood that my BMI score is increasing gradually (32.4). This is quite high. So, to improve my health, I have set an aim to reduce my weight by 5 kilos in 5 weeks and increase my daily walking by 10,000 steps more daily. In this project, I have steed various ways through which I have achieved this aim of mine.
2. Introduction - Why did you choose this project?
a. Problem description
My major problem is my increased body weight. I need to lose some weight since my Body Mass Index (BMI) is much higher than what is considered healthy for someone of my age and height (health.gov.au, 2021). My doctor says that the back discomfort I've been having is related to my weight gain and that my latest blood test reveals an increase in cholesterol. As a result of my recent commitments, I have been too busy to maintain my usual level of physical activity. When I was routinely going to the gym, at least twice a week, I never had the back issues I'm having now. After a consultation with a nutrition specialist, I will also make certain lifestyle adjustments under my power, such as giving up junk food and switching to vegetables and fruits.
This is a major issue. According to data from the World Health Organization (WHO), in 2016, over 1.9 billion adults were overweight, and over 650 million were obese. In the same year, 41 million children under the age of 5 were overweight or obese (Who.int, 2021). The prevalence of obesity has more than tripled since 1975, and it is a major risk factor for several chronic diseases, such as diabetes, heart disease, and certain types of cancer (Who.int, 2021). The increasing prevalence of obesity has been attributed to several factors, including changes in diet, sedentary lifestyles, and environmental factors.
b. Available knowledge
From my problem, I understood that I have a major issue with obesity. Previously I did not know the negative impacts obesity can have on our bodies. After some, I understood that one of the most significant impacts of obesity is an increased risk of chronic diseases such as diabetes, cardiovascular diseases, and certain types of cancer. Obesity can also lead to physical limitations, such as reduced mobility, joint pain, and difficulty performing everyday activities (Gibbons et al. 2019). In addition, obesity can negatively impact mental health, leading to depression, anxiety, and low self-esteem.
c. Rationale
Lewin's Change Management Model is a framework for managing and implementing change within an organisation. The model consists of three stages: unfreezing, changing, and refreezing (Bashori et al. 2020). The unfreezing stage involves preparing anything for change by creating awareness of the need for change and breaking down the existing mindset and habits. During this stage, I will develop my aim to reduce my weight and enter into a healthy lifestyle. The changing stage involves implementing the change, which may involve changes to organisational structure, processes, or culture. During this step, I will change my eating habit and regularly go for a walk to make up to 10000 steps daily. Finally, refreezing involves stabilising the new changes and embedding them into the culture (Cone & Unni, 2020). Under this step, I will make new changes, such as consuming vegan foods and giving up on meat.
d. Aims statement
My proposed aim is to “Reduce my weight by 5 kilos in 5 weeks and increase my daily walking by 10,000 steps more daily”.
3. Methods - What did you do?
a. Context
Previously when I did a check-up, I understood that my BMI score was 32.4, which is higher than a normal person's. With a score above 30.0, I understood that I have obese. A high body mass index (BMI) score indicates being overweight or obese, and it can have several negative impacts on an individual's health. A high BMI can increase the risk of developing chronic health conditions such as heart disease, type 2 diabetes, high blood pressure, stroke, and some types of cancer (Dadar Singh et al. 2022). However, after fulfilling my aim, my BMI score decreased to 26.2. Though it means that I am overweight, I have completed my goal and will focus on having a healthy weight range in the future. To measure my BMI. Firstly I used a scale to measure my weight accurately. Before stepping on the scale, I was sure to remove any heavy clothing, shoes, or accessories. I recorded my weight in kilograms (kg). Then, I used a measuring tape or a wall-mounted height rod to measure my height accurately. Next, I used the following formula to calculate my BMI: BMI = weight (kg) / (height (m))^2. Finally, I interpreted the data and determined my BMI.
b. Intervention/s
To ensure that I can lead a healthy lifestyle, I will take various measures. The interventions include walking 10,000 steps more daily. I will also ensure that I will consume less junk food and healthier food. This will be done by including more fruits and vegetables in my diet. Eating junk food regularly can lead to obesity, which can increase the risk of developing chronic health conditions such as heart disease, type 2 diabetes, high blood pressure, and some types of cancer. Junk food can also negatively impact mental health, leading to depression, anxiety, and low self-esteem. The tools that have been used to measure BMI in this project are digital or analogue scales to measure weight accurately, a measuring tape to measure height accurately, a calculator or a BMI chart to calculate BMI based on the weight and height measurements and BMI apps that use the height and weight inputs to calculate BMI automatically. It is important to note that BMI is not a perfect indicator of an individual's health, as it does not consider factors such as muscle mass, body composition, and overall fitness level. Therefore, it should be used as a general guideline and not as a definitive measure of an individual's health.
c. Measures
I want to keep track of the following for a week or two before I start my 5-week programme to establish a baseline. The data from these items will be used as part of my benchmark.
? My BMI
? Average calories I consume in a day
? Factors include the number of drinks I have each week, the amount of coffee and water I drink, and other things.
? In the course of my normal, regular strolls
? What I eat in terms of produce daily
? My consumption of high-fat, high-sugar, and high-salt meals
I just had a blood test done to get a sense of how my blood is doing right now, and I want to do another one at the end of the five weeks to see if anything has changed.
d. Analysis (if relevant)
From the entire effort given, I have witnessed that, to a certain extent, I was able to improve my health condition. Previously I was obese, but after achieving my aim, I saw that I had become an overweight person. Previously my BMI score was around 32.4, and after achieving my goals, the BMI score reduced to 26.2. My BMI score was reduced by 6.2 scores. This was a huge achievement for me. However, another goal of mine was to walk 10,000 steps more daily. This was not possible for me. With my maximum effort, I could only make up 5000 steps more daily. I tried to control my junk food craving and started having only vegetables and fruits. However, it seemed impossible. So, to please my taste buds, my nutritionist gave me permission to have junk food once a month. In the future, I wish to control all these cravings and keep a target of becoming a healthy person with a normal BMI score.
e. Ethical considerations
Losing weight was a personal goal for me, but ethical considerations need to be taken into account. I ensured that I did not use fad diets or extreme weight loss methods. This is because it can be dangerous and harmful to health. Another ethical consideration is the pressure to conform to societal beauty standards, which can lead to body shaming and discrimination against people who do not fit those standards (Brytek-Matera et al. 2019). Additionally, there is a concern about weight bias and discrimination in healthcare, which can affect the quality of care that individuals receive. It is important to approach weight loss in an ethical and responsible manner, focusing on health and well-being rather than conforming to societal expectations or harmful weight loss methods.
4. Results - What did you find?
BMI
.png)
.png)
Figure 1: BMI Score Improvement
(Source: Author)
The table above shows my improvement in BMI score week-wise. The BMI score in 5 weeks has been stated above. From the graph above, it can be seen that my initial BMI score in week one was 32.4, it can be seen that my BMI score in week two was 31.9, it can be seen that my BMI score in week three was 29.6 it can be seen, that my BMI score in week four was 27.3 and it can be seen that my BMI score in week five was 26.2. From the graph, it can be witnessed that my improvement from week one to week two. However, from week two to week three and week three to week four was quite impressive.
Steps covered
.png)
.png)
Figure 2: Steps Covered
(Source: Author)
The table above shows my improvement in steps covered week-wise. The steps covered in 5 weeks have been stated above. From the graph above, it can be seen that I covered around 2000 steps more daily in week one, it can be seen that I covered around 3210 steps more daily in week two, it can be seen that I covered around 4200 steps more daily in week three, it can be seen that I covered around 3600 steps more daily in week four and it can be seen that I covered around 4980 steps more daily in week five. From the graph, it can be witnessed that my improvement from week one to week two. However, from week two to week three and week three to week four was quite impressive.
5. Discussion – What does it mean?
a. Key findings
Losing weight was a challenging task for me, and it was not uncommon to lack motivation at times. There are various reasons I struggled with motivation when it came to losing weight. It was due to a lack of my self-discipline, not seeing results fast enough, or feeling overwhelmed by the process. The main reason was due to the absence of a support system. Losing weight was challenging, and having a support system of friends or family can make the journey easier. Again, it was due to a lack of enjoyment in the weight loss process. When exercise and healthy eating became a chore, it was easy to lose motivation. Finding an activity or food that I enjoy can make the process more enjoyable and sustainable. It was not uncommon to hit a weight loss plateau, where weight loss stalled even with consistent efforts. This was discouraging and led to a lack of motivation for me. For me, eating is a way to cope with stress, anxiety, or other emotions. Breaking this habit was challenging and led to a lack of motivation. Initially, I did not know how to lose weight effectively, which led to frustration and a lack of motivation. Understanding nutrition and exercise was important for success.
b. Interpretation of results
From the entire process, I have understood the negative impacts of junk food and unhealthy lifestyles that can hamper the human body. With excessive consumption of junk food and an unhealthy diet, I became obese with an increased BMI score of 32.4. From research, I understood that according to my age, my BMI score was quite high compared to normal. So, to focus on my health, I developed a plan and set an aim of losing 5 kilos in 5 weeks. After 5 weeks, from the data presented above, it can be stated that I have improved a lot, although I still have to take more action. However, I witnessed that there are still many areas of improvement that I have to focus on. For example, in week three, my steps covered was 4200, whereas, in week 4, it was around 3600. This reduction in the steps was because of my busy schedule. I was so engrossed in my office that I could not give much time to my health. Due to a meeting, I had to delay my walking time. This issue was resolved in the next week as my steps covered increased to 4980. However, this did not have an impact on my BMI score in week 4 because I kept my diet intact. I did not consume any junk food and only ate vegetables and fruits.
c. Limitations
One of the major challenges that I faced while doing this project was searching for a good nutritionist who could guide me in this journey. Another issue that I faced while doing this project was giving up on my favourite food. This was initially very difficult for me as I used to live on junk foods. Losing weight also required lifestyle changes, such as regular exercise and healthy eating habits. These changes were initially difficult for me to implement and maintain. I also received unsolicited advice from others about their weight loss journey, which can be unwanted and demotivating.
d. Conclusions
This project has positively impacted me as I was able to improve my health and lead a healthy life. I could improve my diet and avoid junk foods that were hampering my health.
Losing weight reduced the risk of chronic conditions and improved my overall health. Carrying excess weight can put stress on joints, making it difficult to move around. Weight loss helped me to reduce this stress, making movement easier and less painful. My back pains were alos reduced. It also helped me to reduce or eliminate sleep disorders, leading to better sleep. I will work to maintain a healthy weight range in the future, even if I am now overweight. I want to become a healthy person with a normal body mass index score in the future by controlling my junk food cravings.
6. Critical reflection
My realisation of how unhealthy my life has been was one of the surprises I encountered throughout this transition journey. Although I've always held the opinion that nutrition has no direct connection with back pain, I was surprised to see that various writers have focused on the causes of back pain (Pasdar et al. 2022). The more I've dedicated myself to making this transformation, the more I've learned about various diseases, and health conditions that I may face in the future or that may enhance the chances of their occurring. As a result, people are more likely to believe that they can avoid the ill effects of any area of their lives by just making an effort to do so.
Over the first three weeks of putting the change into action and treating the issue, I mastered the insights that led to its success via in-depth research and concentration on the main keywords involving health, BMI, contributing factors and causes, and prevention. Pain in the axial lumbosacral region, pain in the radiculopathy, and pain that is transferred from elsewhere in the body are the three most common causes of low back pain (Urits et al. 2019). Back pain affects between 10 and 30 per cent of adults in the United States in any given year. This realisation has motivated me to continue taking preventive measures and making efforts to ensure that I do not become one of the many people whose day-to-day activities are hampered by back pain brought on by the additional weight they are carrying, which is the case for me because of the additional weight I am carrying. (Attention is paid to preventive measures)
In addition to this, I came to the conclusion that before I could consider the new method to be completely functioning, it would need a significant amount of time and effort on my behalf to include all of these new aspects into my routine and maintain a record of them. I neglected to carry out what are known as "initial background studies." I should have spent more time researching the issue before making a change, such as how to take into consideration my age in the transition process or how difficult my exercises would be during the first week due to lactic acid and agonising pain in my body. I should have done this before making a shift. When a change is launched, one of my study interests is to investigate the influence of factors such as social pressures, structural adjustments, and preparation for change (Rogerson et al. 2016).
What went right:
- Results are seen during the first three weeks
- I felt better in general (Back pain, general happiness, and similar)
- There wasn't a lot of variation in the process I mapped.
- As a result of my investigation and implementation of the structured change, I now understand the issue better and am less resistant to future adjustments (Kept my motivation high)
? The responsibility for the transition and the difficulties lay with me.
I feel that I have gotten a great lot of insight into the process, and if I were to do it again, I would probably change it so that it is relevant to a wider range of situations. Despite the fact that the change I decided on is extremely individualised, I would want to expand more while yet being focused on the same topic matter.
If I were to carry out this project once again, there are a few aspects of it that I would change in order to guarantee that I get the results I want and am able to classify it as a triumph.
- Some of my measurement tools may be off, so I will have to upgrade them.
- I want to investigate transformation projects of greater length, during which I expect to include outside parties for advice and guidance.
- Nothing else will be ruled out entirely at this time.
- In the process, I will examine rewards.
- I plan to evaluate a potential shift in my lifestyle on many occasions, taking into account the potential influence of external factors like climate, season, and time of year.
? I'd analyse my plan's immediate and distant outcomes.
In addition to this, I would consider how the medication would influence my eating habits, what kind of assistance from the outside world I might need in order to be really effective if a customised or standard solution would be preferable, and the total cost of the process (Chang et al. 2017).
References
.png)
NUR1203 Cultural Safety and Professional Practice Assignment Help
Brief task description
This assessment task supports you to be an effective Bystander in the workplace and will hopefully extend beyond this. It is a requirement that student nurses and registered nurses are Culturally Safe practitioners. Part of this is when we witness culturally unsafe practice, that we have the skills to navigate this and bring change to the workplace setting.
Length 1500 words +/-10% (word length includes in-text referencing and excludes your reference list and appendices)
Task information
This Assessment requires you to respond to the following case scenario.
You are to identify ONE of the culturally unsafe care points within this scenario and use the four components of the Bystander Intervention Framework as the basis of this essay.
Case study
You are doing a clinical placement on a busy surgical ward, and you are working with a Registered Nurse (RN). Both of you attend to an adult patient, Elliott, who has been admitted for a surgical procedure and requires a blood transfusion intra-operatively. The family identify their religious faith as Jehovah’s Witness, where the belief in the administration of blood and blood products via transfusion is against their faith. Elliott has no vision and is able to communicate using speech.
The RN assumes that Elliott is unable to communicate for himself and talks only to her mother who is in attendance for admission.
The RN turns to face the mother and makes the following comment, “Hello there – who do we have here today? Thanks for bringing Elliott in for his admission. How long has he been unwell for? Do you know? I have his chart here with me and just want to ask you some questions regards his medical history if that’s OK? It says something here about him not consenting to a blood transfusion.... we’ll need to sort that out, because he’s going to need it you know!”
After finishing off admitting Elliott to the ward, you walk back to the nurse’s station with the RN. The RN turns to you and states “What a weird religion that stops you from having a blood transfusion. Why would anyone want to be in that religion?”.
1. Identify ONE of the culturally unsafe care points and explain its relevance to this case study and explain why it is culturally unsafe.
2. Identify 2 Direct interventions that you could use in this scenario. Your response cannot be a replication of any responses that have been provided with, in your Bystander training
3. Identify 2 Indirect interventions that you could use in this scenario. Your response cannot be a replication of any responses that have been provided in your Bystander training.
4. Identify 2 Distraction interventions that you could use in this scenario. Your response cannot be a replication of any responses that have been provided in your Bystander training.
5. Protocol intervention/s: Identify the NMBA Codes of Conduct that this culturally unsafe care is breaching.
Writing Style
• This assessment piece to be written as an report and in third person.
• Do not use headings
• Correct Academic writing as per USQ guidelines
• All discussion is to be appropriately referenced using APA 7th Edition Referencing
• Contemporary Literature must be sourced (no more than 7 years old).
Solution
Introduction
As per professional standards for registered nurses (RN), nurses must reflect dignity and professionalism through their practice and ensure patient right over person-centred and well-informed treatment practice. This report focuses on identifying culturally unsafe care reflected by RN in the case of Elliot, who belonged to Jehova's Witness believers and denied blood transfusion as per religious belief. This report also highlights 2 direct interventions for this case and 2 indirect interventions for this case, and 2 distracting interventions for nursing assignment help.
Culturally unsafe care points
In the case of Elliot, culturally unsafe care practice has been witnessed by an in terms RN responsible for the care of patients disrespecting the religious belief of the patient for not consenting to intra-operative blood transfusion rather than making the patient and family members of the patient agree on the procedure through empathy. The RN has also breached patients' right to the confidentiality of personal information as RN has communicated about patients' religious beliefs and treatment outcomes openly in nurse stations and reflects disrespect towards the religion. As mentioned by Poorchangizi et al. (2019), nurses have the responsibility of safeguarding patients' right to confidentiality. This right has been breached here by the RN, along with disrespect to the patients' culture. The RN has also avoided directly communicating with the patient even though the patient can talk. These are the areas where RN has reflected culturally unsafe care practices, lack of dignified behaviour, and respect towards patients' cultural needs and health conditions. This incident reflected unprofessional behaviour by the RN's breach of patients’ rights.
Direct intervention
The case here is to ensure a culturally safe care environment for Elliot. Direct interventions that can be considered in this case include training RN to deliver care in a culturally competent manner and ensuring collaboration with community health service providers. Authority of care service-providing organisations can consider arranging training for RN to enhance their cultural competence. Cultural competence among nurses can be enhanced by making them aware of different cultures and the importance of reflecting respect for the culture and religion of patients in the nursing profession (Kaihlanen et al., 2019). For example, during training sessions, the RN can be made aware of legal consequences associated with not respecting the religion of a patient, as well as improve the RN's ability to communicate with patients in a culturally competent way for incorporating changes in the RN's behaviour. Further such training can also improve other RNs' perception regarding the importance of maintaining culturally safe care practices to avoid the recurrence of such incidents.
On the other hand, including community healthcare professionals in the care team of Elliot can be beneficial for reducing the cultural barrier in care. The main concern here is no consent for the intraoperative blood transfusion, which is necessary for the patient. Community health service professionals can communicate with the patient and his family to make them understand the consequences of which blood transfusion becomes necessary during treatment and ways the patient can avoid breaching their religious values without impairing the treatment requirement (Bolcato et al. 2021). The community health professional can also help RN to understand patients' perspectives associated with treatment measures that can help to solve complications associated with the treatment plan
Indirect interventions
As the RN has reflected on culturally unsafe behaviour in terms of not respecting the cultural beliefs of patients and not prioritising patient confidentiality, strict measures can be taken against RN by making management aware of the situation. Further, appointing a different RN with professional knowledge of cultural competence and knowledge of managing patients with Jehovah’s Witness beliefs can be beneficial. RN can lose their license and job for not following professional standards and ensuring respect toward the cultural needs of patients. As mentioned by Handke et al. (2019), cultural competencies-related practices in healthcare settings allow limiting cultural disparities associated with treatment specification and help to minimise the consequences of inequality. Thus the respective case reflecting the poor understanding of cultural competencies highlights the presence of inequality in the case of the patient belonging from a significant religious belief only for not providing consent to a treatment requirement. Thus making authorities aware of the situation and taking strict action against the RN can help to limit the recurrence of such a situation in the future.
As the current RN appointed for Elliot has reflected a poor understanding of cultural competence thus, another RN having profound knowledge about the requirements of cultural competency can be appointed to manage this case. Ensuring a cultural competence care environment for the patient can help to limit the cultural barriers arising in the treatment plan as well as the dignity of the patient can be maintained. Further, replacing the existing nurse with an experienced professional will provide understanding regarding patients’ consent redefining other treatment methods that can be applied to replace the intraoperative blood transfusion. Thus it can be considered a strategy for dealing with the current situation.
Distracting intervention
Application of cognitive behavioural therapy (CBT) and counseling sessions with family members of patients in the presence of community service providers knowing dealing with issues of care associated with a patient with Jehovah’s faith can be considered in this case. As mentioned by Babiano-Espinosa et al. (2019), CBT allows the development of an interacting treatment environment for service users and service providers for better delegation and patient care needs. In the current case of Ellitor thus CBT based approach can be applied to reduce resistance to blood transfusion. Under this approach safety of blood transfusion in terms of their religious values and consequences for not considering the blood transfusion can be communicated. The CBT approach focuses on including changes in the behaviour of patients by encouraging and guiding them to judge a situation from a positive side. Thus this technique can be beneficial for making Elliot and his family members provide consent for blood transfusion.
A set of counseling sessions can be arranged for Elliot and his family members, and during the secession, it will be ensured that privacy and confidentiality are maintained. During the counseling session, it can be ensured that the patient and the family members actively participate in the communication to clarify the issues of not considering blood transfusion and the current health condition. Such sessions can also be used for reforming their existing experience due to poor behaviour of RN to ensure the trust of the patient and his family member over the services provider. It will help to ensure a cultural safety care environment and limit the issues associated with consent.
Protocol interventions
NMBA code of professional conduct forces nurses' duty to ensure patients' rights and respect for patients' decisions. In this respective case of Elliot, there are certain arise that RN has avoided and neglected. The first area neglected was the patient's condition, as Elliot could speak; however, the RN preferred to communicate with his family rather than the patient, which highlighted impairing patient-centered practice and informed-making. This activity of RN breaches the first code of conduct of NMBA, which is focused on nurses' practice safely and competently. As per this code of conduct, nurses must act safely and competently without being compromised by patient health limitations (Nursing and Midwifery Board of Australia, 2022). In this case, RN neglected Elliot’s personal views on the matter of blood transfusion though can communicate this code of conduct 1 has been breached. Code of conduct 4 NMBA standard focuses on ensuring nurses respect and dignity towards patients' culture, ethnicity, and values as well as beliefs while receiving care (Nursing and Midwifery Board of Australia, 2022). However, in this case, Elliot, while communicating with his family member RN considered a very informal way of communicating, reflecting the less interest in the patient's cultural and religious identity.
Further, while communicating with other RN, the respective nurse became very disrespectful to Jehovah's Witness's religious beliefs by saying the religion was weird and questioning the following religion. This incident signifies disrespecting the cultural and religious identity of the patient, thus breaching the code of conduct 4 of NMBA standards. Code of conduct 5 has also been breached in this unsafe cultural practice as this code highlights nurses' responsibility to maintain the confidentiality of the personal information of patients as per the National privacy principle 2001 and Privacy Act 1988 (Nursing and Midwifery Board of Australia, 2022). However, the RN, in this case, avoids confidentiality of the patient's details, such as cultural and religious specifications, by openly communicating about it in the nurse station. This code of conduct 5 of the NMBA standard has been breached in this culturally unsafe practice.
Conclusion
Thus it can be concluded that here RN has breached the NMBA code of conduct 1, 4, and 5 through culturally unsafe practice. The issue that arises can be solved through training sessions to improve RNs' knowledge regarding cultural competencies and CBT, as well as community healthcare service providers' engagement for making such patients and their families actively involved with care requirements. These techniques can help to ensure patient rights without impairing treatment specifications.
References
.png)
NURBN2025 The Health and Cultural Diversity Assignment Sample
Assessment Description:
Students to explore impacts to health and health outcomes for Aboriginal and Torres Strait Islander Peoples, as well as demonstrate the importance of incorporating cultural perspectives in clinical practice as future healthcare professionals.
Overview:
The purpose of this task is to demonstrate cultural safety in clinical practice. You will critically examine a case study identifying the necessity of culturally safe practice to improve the health and health outcomes for Aboriginal and Torres Strait Islander Peoples.
In assessment task 1 you identified an understanding of your own identity, along with social and cultural factors and how this has influenced your own beliefs about, and interactions with, Aboriginal and/or Torres Strait Islander Peoples. In this assessment task you have the opportunity to apply this self-reflection to practice when exploring the events of the following case study. Your responses are to be evidence-based.
Case Study
Annie is a 59 year old Aboriginal women from the Atherton table lands near Cairns, in north Queensland. Annie is passionate about being an Aboriginal community member, enjoying yarning with her community and attending local community events. Annie has one daughter Sharelle, 32 years old and one son Tony, 30 years old. Sharelle has 3 children, Sarah 12 years old, Kelly 9 years old and Alex who is 3 years old. Sharelle lives close to Annie in the Atherton Table lands.
Annie has lived independently for many years and was employed as a Murri Primary School Teacher which she loved. Annie retired 3 years ago to support her daughter with caring for her children. Annie had separated from the father of Sharelle and Tony many years ago.
Annie is visiting her son Tony and daughter-in-law Kate in Melbourne (within the Monash health catchment area). They have a baby, Lily who is 9 months old. Kate is returning to work so Annie has come to Melbourne for an extended stay to help care for baby. Annie enjoys caring for and getting to know Lily. Lily is relatively easy to look after, sleeping through the night. Annie takes over the care of Lily once Tony and Kate go to work. Annie loves signing songs to Lily. She also takes on the usual care like feeding and changing nappies. Lily will sleep about 3 hours in the middle of the day, so this gives Annie time to rest or tidy the house. Annie will take Lily for a walk if it is warm enough once she wakes up. Tony and Kate will take over the home tasks when they arrive home from work.
Annie is a bit lonely as she does not really know anyone. Annie is missing the mob in the Aboriginal Planned Activity Group where she is involved in yarning, gardening and walking activities. Annie’s favourite was art as she was creating a piece for a local exhibition. Annie does not like hospitals; she has a fear of hospitals because her community have had bad experiences.
Case Study Instructions
Move through this case study by addressing the following situations:
Section one: How do you ensure you are committed to a journey of cultural safety?
You are on a morning shift at Dandenong Hospital, Monash Health and have been informed that you need to admit a patient being transferred from the Emergency
Department. You receive the handover:
Annie is a 59 year old Aboriginal women from the Atherton table lands and has Type 2 diabetes and Hypertension, diagnosed when she was 50. She has managed her diabetes with the support of the
Local Aboriginal Health Service (Wuchopperen Health Service Limited:
https://www.wuchopperen.org.au/health-support). Annie had been informed that her kidney function was deteriorating which she had been following up at this service. Shortly after arrival in Melbourne Annie becomes unwell and is admitted to hospital. Annie was experiencing intense ear pain and had become very unsteady on her feet, later diagnosed with a severe ear infection requiring intensive intravenous antibiotic treatment.
Annie arrives on the ward; you greet Annie while taking her to her bed. How do you ensure you are committed to a journey of cultural safety?
1. Provide an evidenced based strategy that enables you to continue your cultural safety journey.
2. How do you welcome Annie into the ward?
3. Annie reveals her current situation with you, as outlined in the case study. What actions would you take following this conversation? You are advised to investigate an Aboriginal Community Controlled Health Service that would be able to support Annie while she is staying in Melbourne.
Section two: Addressing culturally unsafe practice.
You are now at handover. You are presenting Annie to the nursing team. You have just described Annie’s symptoms. You have said Annie is very unsteady on her feet and before you can continue you hear two nursing colleagues say, “I bet she’s an alcoholic. We will make sure we limit her pain relief”. To unpack this situation please answer the following questions
1. In NURBN2025 you were introduced to racism, the causes and impact on health outcomes Identify from peer reviewed literature the possible reasons why non-Indigenous people make racist assumptions about First Nations peoples. Include the following:
a. The potential beliefs, values and attitudes that have influenced these non- Indigenous nurses to be culturally unsafe.
b. Describe how these nurses have used power differentials related to their beliefs, for nursing care.
2. How would you advocate for Annie in this handover?
Section three: Promoting Cultural safety
You make an appointment to meet with your nurse unit manager (NUM) to address this culturally unsafe practice. What team based solutions could you present to your NUM. Think of this in terms of:
1. How could cultural safety be promoted within this ward?
a. What antiracist group learning strategies could be implemented?
b. How could power differentials be minimised?
Please note the word counts are a guide. The reference list is not included in the word count.
Solution
Section 1:How do you ensure you are committed to a journey of cultural safety?
The case scenario conveys that Annie is afraid of hospitals as her community has had a bad experience with care services. It is very common that Aboriginal and Torres Strait Islander patients mostly confront several issues or challenges as the medical practices including nurses and doctors carry biased attitudes toward the community (Arrow et al. 2018). Thereby for a patient like Annie confirming cultural safety and equality in accessing healthcare is very important to confirm a safe environment for the healthcare setting. In order to confirm cultural safety for Annie, stakeholder engagement is much more important to confirm openness, respect, and offer safe care to a patient like Annie. It can justify a trustworthy, flexible, respectful relationship during the period of treatment. In order to confirm cultural safety, maintaining the privacy and secrecy of the patient is another important consideration as most of the aboriginal people do not have such type of offering during their intervention in the healthcare setting for best assignment help.
Considering Annie's fear regarding her healthcare setup, it is very important to welcome her to the ward with all warmth confirming a friendly environment. It would even help to justify cultural safety in the process. The nurse needs to be skilled and professional enough to carry an unbiased attitude and treat them in the same way as other patients. A welcoming attitude can even be confirmed by behavioral attempts where maintaining eye contact can offer assurance to Annie to be comfortable in the setup. Cultural safety can even be accommodated in the practice through effective communication where more focus would be on listening as most effective communication is mistaken by speaking. More listening to patients like Annie can help the nurse to be more acknowledged of her culture, and background to address her needs accordingly. It would help to sustain cultural safety in the setup. Before proceeding with any intervention for her difficulties taking her decision and discussing the intervention procedure with her is a must to avoid ethical issues like informed consent, autonomy, etc (Beks et al. 2019). Addressing to the referred ethical issues can even help to sustain a positive, safe, cultural environment in the healthcare setup. Having an understanding of Annie's difficulties as well as cultural considerations, it would be better for the nurses to arrange a support system to confirm that her main health issue is being addressed.
Annie does not have an extended family to help her out and her son and daughter might not be that much effective to offer her support. Thereby to confirm her continuous improvement regarding all types of health issues, it will be better to take the help of community services so that she can recover first. Annie is already getting the help of services to manage her diabetes but the service is not available in Melbourne as it belongs to Queensland and Annie is in Melbourne right now. Thereby it is important to arrange for another type of health service for Annie which is available and accessible in Melbourne. The help of any local aboriginal network can be communicated to confirm cultural safety afterward. As this particular network would help to be connected with the support service for the community; thereby it would be a better consideration to confirm cultural safety. The service needs to be such where several segments like raising awareness, building partnerships, information determination, etc which would be much helpful for Annie to be self-dependent in all terms. There are services like ACCHO and NACCHO that can help Annie in her situation through their programs and policies (Bovill et al. 2021). It would even help her to get rid of her fear of hospital services as these particular support services are for the community she belongs to and it is definitely help her to be comfortable and feel culturally safe and secure in all terms.
Section 2: Addressing culturally unsafe practice
In legal considerations, it has been confirmed in Australia that equality would be there in the health sector with no discrimination for race, gender, background, tradition, custom, etc. However, the practical scenario does not get properly aligned with the same; rather there are several nonindigenous people who consider aboriginal and Torres Strait Islander people as discriminated, against, and unequal, and make them marginalized. It can be confirmed undauntedly that everyone has their own attitude, value, and beliefs but individualism should not lead to racism including hatred, discrimination, or prejudice due to their origin, or color. It even extracts the negative image of the sector as well as the societal structure of the country. Health Care sector belongs to emergency services and racism cannot be overflowing in such a sector; still, nurses often exercise power differentials as per their values, belief, or attitude. They often ignore Aboriginal and Torres Strait Islander people and do not pay proper attention to their symptoms to offer them safe care intervention (Jayakody et al. 2020). Such a type of attitude immediately confirms culturally unsafe practice on the part of the nurses. Most of nonindigenous nurses believe that aboriginal people can be only one community and there cannot be any variation regarding that. However, that is a complete misconception regarding aboriginals which eventually leads to improper addressing of cultural diversity followed by culturally unsafe practices. Furthermore, most of the non-indigenous people believe that aboriginals or indigenous people are illiterate, ill-mannered and live a gross life where they always get involved with drinking, smoking, and the use of drugs. Research even confirms that they are not very interested to work but rather always ask for everything for free. Such type of wrong information or improper belief regarding indigenous people on the part of non-indigenous people eventually attracts unsafe practice by creating a barrier in the care intervention (O’Donnell et al. 2020). Due to such type of wrong beliefs, nurses often do not share enough concern or focus for the patients or their symptoms and rather carry a biased attitude which becomes the main barrier for the entire care process. Such a type of attitude will definitely make Annie very uncomfortable, hurt, and angry due to the involved discrimination. She can even think of racist activities in the health care center which eventually can increase her uncomfortable regarding the healthcare setting. Thereby, it would be better for the nurses to exercise an open flexible environment in the setup. It is even important to exercise effective communication and shared decision-making in the process where the patient like Annie would not feel left out but rather can play an active role in the entire intervention. As the nurses of the next shift have a misconception regarding the aboriginal community and already have confirmed their biased attitude towards Annie, thereby, it is important for the nurse of the present shift to make them aware of some important considerations while the handover. It is very important to convey human rights, patient rights, and several ethical issues to be followed by the nurses during handover to assure or informed them about consequences. It would help them to be more focused on the patient without sharing any biased attitude toward her aboriginal background. It would be even more relevant if the nurse on the present shift would convey her experience with Annie (Quinn, 2019). Such information can remove the misconceptions of the nurses conveying the fact that all aboriginals are not involved in features like smoking, drinking, taking the drug, etc to confirm a culturally safe environment for Annie.
Section 3: Promoting Cultural safety
Such unfair practices need to be stopped as well as promoting cultural safety is another important consideration to be taken care of. In order to promote cultural safety in the hospital care setting, the nurse unit manager needs to be conveyed of such unfair practices. Apart from conveying the thing, it is even important to take some initiative to promote cultural safety. The first and foremost concern to promote cultural safety in the practice can be training (Skoss et al. 2021). Training would be much helpful to make the nurses informed or acknowledge about cultural diversity. The training can make them more efficient, skilled, and effective to remove the issue of cultural diversity and promote
cultural safety. If the nurses of the next shift had enough information about aboriginals then they might not have such type of generalized attitude or behavior towards Annie rather they can secure a friendly safe environment for her treatment. Hence, it immediately can confirm cultural safety in the process. Decision makers and nurses in the healthcare sector are the main stakeholders to exercise or initiate action to attain sustainability as well as success for their efforts. There are some nursing principles and foundations to avoid ethical issues. The training even needs to accommodate the same so that the nurses would have enough knowledge regarding informed consent, authority, non-maleficence, and beneficence which eventually would help them to avoid improper addressing to the patient and automatically culturally safe practice will be aligned in the setup (Tremblay et al. 2020). The training even needs to convey the consequences of otherwise situations to make the nurses aware of all positive and negative to secure cultural safety in the process.
References
.png)
NRSG367 Transition to Professional Nursing Assignment Sample
Assessment Task Overview
Critically analyse the following case study to answer the essay questions.
Case Study Background
Harry is a Graduate Registered Nurse (RN) who is 8 weeks into his first graduate rotation at the local metropolitan, tertiary hospital. He is currently working on a Medical Ward. For the first four weeks Harry worked alongside his nurse preceptor, predominately rostered on morning shifts. Harry has just completed his first five (5) night shifts yesterday morning and is back on an afternoon shift today (Saturday).
Harry is still trying to manage his roster and other commitments like social touch football with his friends and mountain biking. Today, Harry is feeling tired and frustrated because he slept through his alarm this morning and missed his sister’s birthday breakfast celebration. He is also disappointed that he can’t join his team for the touch football end of season breakup in the evening.
On Shift
Harry has arrived 15 minutes prior to this shift starting. On arrival, he realises that he hasn’t worked with the Nurse-in-Charge before but there are other nurses on the shift that he has met.
Harry feels a little nervous, but he knows two (2) of the patients he has been allocated from his recent night shifts and he is allocated a further two (2) patients who are to be discharged this afternoon. He has not arranged a discharge before so he prioritises these activities as he prepares his shift planner.
A short time later the Nurse-in-Charge tells him that his patient allocations have changed due to skill mix. A different nurse will arrange one (1) patient discharge and Harry will be receiving a new patient from Emergency Department.
Harry feels overwhelmed with the admissions and discharge. He is unsure how he will cope with the rest of his shift. Harry has not looked after a patient (Mr Somersby) who is confused, high risk of falls and wanders around the ward. He is reluctant to ask the Nurse in Charge for assistance as he does not want to appear ‘incompetent’. He decides he must push on, and soon it is time for handover.
At handover, Harry realises that after he had not given Mrs Williams her IVAB. To help with his time management, Harry had set the observation machine to take automatic observations. However, he had forgotten to go in and check this patient for the last 3 hours. Harry has not yet completed the admission documentation for Mr Sommersby as he has been trying to stop him from wandering out of the ward.
Additionally, he has not completed any of his patient notes on the computer on wheels (COWS) machine. The nurse he his handing over to rolls her eyes when this information is handed over. Harry stays 30 minutes after the end of his shift to complete his work.
Following his shift
On his commute home, Harry feels anxious and feels that he did not provide sufficient care for his patients, in particular Mrs Williams. He is frustrated with himself that he may have missed other things this shift and that he had to stay late to finish his patient notes. At home, he spends some time reflecting on his shift and plans to ask his nurse preceptor for any advice/tips on their next shift together.
Harry appears to be struggling during his clinical shift. He also seems to be having difficulty maintaining a work/life balance. Critically analyse the provided case study to answer all the following three questions within an essay format:
1. Determine and justify whether the graduate RN met (or did not meet) their role and responsibilities as an RN during his shift. Provide at least two (2) case study examples and support your discussion using evidence, including Nursing and Midwifery Board Australia (NMBA) Registered Nurse Practice Standards (2016).
2. Construct at least three (3) recommendations as to how the graduate RN could have undertaken this shift differently. Consider in your discussion the knowledge, skills and attitudes inherent in the RN role, including utilisation of technology and teamwork skills, and support your discussion with literature .
3. Transitioning from student to Graduate Registered Nurse can be difficult. Construct at least two (2) evidence-based strategies that could be implemented to promote resilience, build capacity, and support work/life balance during the graduate RN’s transition period .
Instructions:
• Word limit is 1800 words (+/- 10%), including the introduction and conclusion.
• Paper to be written in essay format, must answer the above questions, and should be written in academic writing style (not first person). You may use headings.
• Ensure you consider the AT2 Rubric, Appendix 2 in the Unit Outline, when undertaking this assessment task.
• Submit your paper to Turnitin by the due date.
Solution
INTRODUCTION
This study will answer three questions based on a case study for assignment help in which Harry failed to perform his Registered Nurse (RN) role. This will also examine the negative examples that have made Harry agitated due to his poor performance in this workplace and taking proper care of patients assigned to him. Moreover, some recommendations will also be given along with strategies that help Harry balance his work and personal life.
DISCUSSION
Meeting the RN Role
Harry is a newly appointed graduate Registered Nurse who joined his workplace 8 weeks prior. He was assigned his duty during the morning shift and was suddenly given night shifts and again allotted an afternoon shift the next day. This has made some issues for Harry in balancing a professional and personal life. Moreover, time management was one of Harry's biggest challenges that impacted his working pattern. The day when Harry was allotted an afternoon shift, Harry was depressed and agitated because he wanted to join a football match; however, due to his duty, he had to miss that match. This has impacted his professional life as he has failed in appropriately playing his duty. Work and personal life balance help a person to enhance the level of productivity that helps in career development (Zhu et al., 2022). Due to a lack of time management, a skill that every RN must possess, Harry has failed to take care of his allotted patients. He has failed to give proper medication to Mrs. William. Lack of Time Management is one such negative example of Harry as he has failed to balance his personal and professional life properly, failing to attend the football match. It is significant to note that time management is quite important for RN in getting huge success in their career (Popejoy et al., 2022). Another negative example was that Harry failed to look after Mr. Somersby, who has a high fall risk. Harry was confused and even failed to ask the head nurse for help.
Mr. Somersby would receive proper treatment.
Notably, a registered nurses role is to coordinate the treatment and care of every convalescent. Their responsibilities also vary from drawing blood and educating convalescents regarding their health (Henshall et al., 2018). An example of the case study given in the Nurse and Midwifery Board of Australia is that Ms. Jaclyn Stratton, who was working as a psychiatric nurse, was suspended from her job role as she failed to diagnose the vulnerability of the patient with whom she was dealing. It is important to note that she has failed to perform her duty as she needs to balance her personal and professional life properly. One of the biggest responsibilities RNs play is assessing, observing, and speaking to the convalescents regarding their health issues (Halcomb, Smyth & McInnes, 2018). They are also responsible for recording the symptoms of the ailments, results of the diagnosis and all other essential records regarding the patient's history (Mahoney et al., 2020). Preparing the patients for operations and various tests and offering them essential treatment facilities and care is also a significant duty of an RN. It was also found in one of the case studies in 2018 that two people die due to poor performance standards of registered nurses. The family members of the dead persons have complained that one of the registered nurses was responsible for providing the wrong medication and that impairment has taken away the lives of two people (Chang & Daly, 2016). According to the Nurse and Midwifery Board of Australia, professional conduct is concerned with significant values that can be easily outlined in the set of obligations; codes of midwives and nurses must be prepared for explaining and justifying the actions and decisions. Nurses offer services to the convalescents to be easily cured of their ailments. A lack of time management and balancing work/life are the biggest reasons registered nurses become agitated and fail in performing their job roles (Nursing and Midwifery Board of Australia, 2018).
Moreover, they must possess certain skills which are significant in maintaining patients' health and giving them better healthcare and treatment amenities. Harry lacks one of the basic skills that every RN must possess: emergency assistance in medical care. When Mr. Somersby's condition deteriorated atrociously, he failed to call for emergency help so that he would be able to give him better treatment. Rather he remained silent and did not ask for help, which could have taken away the life of Mr. Somersby.
Recommendations for Harry to improve his skills as an RN
The following recommendations are given so that Harry can improve their time management skills and give proper treatment facilities to the patients. This includes emergency cases when the health of the convalescent deteriorates.
Teamwork in nursing is concerned with patient-centric behaviour focused on accomplishing targets working with other nurses (Rosen et al., 2018). Harry must learn to work within a team as it will help give proper care facilities to the convalescents. It also helps in enhancing the standards of outcomes for the patients. Hence, the major motive of the teams in healthcare must work in a team to make other nursing staff learn how to provide high standards of healthcare amenities that aid a patient receiving from ailments (McLeod et al., 2021). Nurses are required to purposefully integrate teamwork and their working patterns to further assist in seeing better responses from the patients and more enhanced accomplishment of the goals.
Registered nurses must work together in collaboration that helps develop solid safety and security outcomes for patients. In addition, it is recommended that when registered nurses work in collaboration, it helps improve the level of communication and productivity of these nurses and helps the healthcare centers to gain maximum benefit in the competitive edge (Zajac et al., 2021). This will help Harry improve his conversation skills with other nurses, which will help reduce his nervousness and enable him to approach other nurses without fear when an emergency occurs. This also helps improve strong nursing care facilities and interdisciplinary linkages (Herzberg et al., 2019). Teamwork skills must be learned so that the efficiency standards can be enhanced in caring for the convalescents, which leads to more brand awareness of the healthcare institutes and more competitive advantage.
It can be concluded that Harry, a registered nurse, must develop certain skills so that he can be able to provide better healthcare facilities to the patients. It is also analysed that better communication standards, developing resilience and using digital technologies must help healthcare professionals in providing better services and it also helps personal development.
Reference list
.png)
NRSG374 Principles of Nursing Assignment Sample
Assignment Detail:
Students are to provide an 1800 word critique of the provided case study using only ONE CPG.
To complete this task you will need to discuss and critique relevant elements of the CPG and case study whilst upholding the National Palliative Care Standards at least one of:
- NSQHS
- NMBA standards and/or
Assessment criteria: The assessment will be marked using the criteria-based rubric.Please note that in-text citations are included in the word count whilst the reference list is not included in the word count. Words that are more than 10% over the word count will not be considered
Now that you have read the case study and selected ONE of the CPG provided you are required to:
- Review and critique the care given to the patient against the CPG you have selected and provide evidence to support your critique through additional research that you will undertake
- Highlight the importance of the National Palliative Care Standards and at least one of the NSQHSS and/or the NMBA Standards and how they influence our practice
- Demonstrate knowledge on the illness trajectory of Motor Neurone Disease (MND) in line with Palliative Care Principles
- Provide links between the case study and your chosen CPG to identify highlights or limitations in care
- Ensure that your sources are all contemporary (within the last five years) and from evidence based sources)
- Read all instructions and the rubric very carefully
Case study – Care of the dying patient CPG
.png)
.png)
Solution
Introduction
Palliative care is a type of care that is a person and its family-centred care with a progressive, active, advanced disease who is going to die or has such prospects of cure. The goal of this type of treatment is to maintain as well as optimize the quality of life (Cheluvappa & Selvendran, 2022). On the other hand, there is a need to mention that the Palliative Care of Australia stated that the chosen palliative care must be strongly responsive to the needs of the diseased person and their family. On the other hand it also strictly considers that all living persons must be provided with the respective care for advanced, progressive diseases and also regardless of the diagnosis (Borbasi et al., 2019). In the respective case study of Tyler, there is palliative care provided by the palliative care team as per his wish, the respective report is trying to critically evaluate CPG with the usage of an appropriate standard to provide the respective person more support and also help his family.
Chosen Clinical Practice Guidelines or CPG with Reason
First of all, there is a need to understand Motor Neuron disease, the illness trajectory of motor neuron disease and the patient's background. In the case of the respective disease of MND, death takes place within a year of diagnosis in most cases and in some cases, it takes two years (Brown et al., 2017). On the other hand Mr Tyler is a young man as his age is only 40 years and has a nice family, so there is a need to consider the EBP means the evidence-based practice and also appropriate standard of care to provide END of life care CPG (Wardle et al., 2019). The respective CPG is that Tyler's death is really unexpected for his family. His babies are too young and he just started his journey of life only a few years ago. On the other hand, Tyler wants to spend quality time with his family as he knows about the disease; he also wants his family reunited though he is not there with his family in future. Sixt, considering all this, there is a chosen END of life care CPG takes place to provide appropriate palliative care to Tyler.
Demonstrate knowledge on the illness trajectory of Motor Neurone Disease
(MND) in line with Palliative Care Principles
Motor neurone disease or MND is a type of progressive disease related to the neurology of a person. The respective disease leads to paralysis in hand, leg. As times go there are the issues of swallowing and problems of breathing also develop in the patient of respective disease (Oliver et al., 2020). As per the principles of the Palliative care, the care always is patient, family and carer centred, so it is able to provide support to Tyler to get appropriate care as well as of to his family and also to carer. On the other hand it is also based on the assessed need. It was the desire of Tyler that his family must be reunited before his death and he can die with honor that must be provided by the palliative care. On the other hand, Palliative care also ensures that the patient, family and carer get the help of local networked services, as per the respective case study Tyler and his family get the help of the local network. On the other hand, palliative care always ensures that the treatment must be evidence-based, clinically and culturally safe. The trajectory of Motor Neuron Disease always needs to be considered. Care is integrated and coordinated, that is also the principle of Palliative care. The integrated and coordinated care supports the patient of motor neuron disease to get physical and mental relief. The sixth principle is in palliative care there is also a clear understanding developed between the care provider team and the patient and his or her family to understand what is the meaning of the care to each of them (Oliver et al., 2020) . So for the respective case study there is at first clear understanding that must be needed to develop what is the meaning of palliative care for Tyler, Catherine and also for the other family members.
Critical Evaluation of the applied care
The respective palliative care that is provided to Tayler needs to consider not only the care of the respective diseased person there are also need to consider the condition of the family members also (Palliative Care Australia, 2018). Because the Australian Palliative Care stated that there is a need to include the care of the family of the ill person also in the respective care (Abbott et al., 2020). Through the case study, it is visible that there are conflicts among the Joycee which means the mother of Tyler and the wife of Tyler means Catherine. On the other hand, it is their wish of Tyler that his children also consider his situation before his death so that he can spend quality time with his family. But such initiatives take place from the side of the Palliative care team, due to the fact that at the end of his life he cannot get his all family members together and close to him except his wife. On the other hand, it is the duty of the registered nurse to provide Evidence-based nursing and consultative nursing and promotion of health and do holistic assessments (Sharplin et al., 2020). In the respective case study, also needs to mention that no such usage of the SAS tool takes place. According to Heslop (2019), SAS tools mean the Symptoms Assessment scale is supportive to understand breathing, pain, insomnia, appetite problems, nausea, fatigue and so on together. On the other hand as per the guideline of the PCOC the usage of the SAS tool is important to measure the appropriate cause by understanding the most important seven symptoms (Eagar, Clapham & Allingham, 2020). There is also a need to consider the Problem Severity score on the time of providing the palliative care to the patient that is also not considered the respective case study and the palliative care team to handle the case of Tayler. Basically, the 4 - point scale is used to understand pain, family problems, spiritual family and so on (Tian et al., 2020). The measurements that take place are either absent, mild, moderate or severe through the respective scale. Hereby also need to include that there is no such usage of the karnofsky Score also takes place within palliative care (Kolakshyapati et al., 2018). The respective score is effective to understand the capability of a diseased person to do some common activity based on the care also provided to increase in quality of life of the family members as well as of the affected person.
NSQHS
The registered nurse has a crucial role in preventive, socio-cultural, therapeutic and also in the promotion of quality patient-centred and family centred palliative care. The World Health Organisation also considers palliative care as an approach that is able to improve the life of patients whether they are adults or children also to their families, especially in the case of life-threatening diseases (Australian Commission on Safety and Quality in Health Care, 2020). On the other hand as per the view of Palliative Care of Australia the Registered nurse plays one of the important roles in the case of providing the END of Life care. The respective care is included with appropriate goals, advanced care planning and monitoring with the appropriate acknowledgement that the patient is improving or not. The National Palliative care of Australia is supported by the nine standards that need to be considered by any registered nurse during the time of providing Palliative Care to a patient. On the other hand the National Safety and Quality Health services provide the appropriate support to the patient (Ritchie et al., 2018). On the other hand, there is also a need to mention that the consideration of NSQHS was also chosen as it in some of the case overlaps with the NMBA nursing standard. This Means NSQHS is able to provide proper care to the patient by maintaining the respective standard.
.png)
Figure 1: National Palliative Care Standards
(Source: Cheluvappa & Selvendran, 2022)
Highlights
If the respective standard is considered by the registered nurse at the time of providing care to Tayler about the Palliative care then continuous changes take place within the developed plan as deterioration takes place in the case of the affected person. On the other hand there are psychological, metaphysical theological and emotional aspects that help Tayler to manage his grief and he may be able to give strength to his family members by reuniting them. As per the respective and considered standard once a patient is identified that due to disease the person is going to be dying soon then appropriate terminal care is provided to the patient. All the spiritual convictions and preferences of the affected person must be considered by the respective standard. So it can be stated that implementation of the NSQHS standard is able to support Tayler to fulfil all his wishes about his family before his death, ultimately able to complete the End of life care CPG. The treatment of Tayler must be incorporated with ACP means the Advanced Care plan, Medical treatment decision maker and Advanced care document ( Cheluvappa & Selvendran, 2022). There is the selection of the final rites, final venues also take place. In the case study it is recognised that the recommendation takes place from the side of the Medical Officer to admit in the hospital though Tayler was not interested in that.
Application of standard 2 of Quality and Safety Management as per the case of Tyler cover underlying theme was "Partnering with Consumers," which necessities for efficient execution of the medical field dealing directly with patients. The foundation for quality and security is laid forth in Standard 2 (Quality Health Service, 2022). Thus, by laying up the typical organizational features and operational flow inside a secure institution adequate palliative care could be given as per NSQHS. Partnering with Tyler standard calls for efficient and relevant patient participation in reviewing, designing, and deployment of services, given that evidence supports doing so that indicates patient participation may lead to enhanced reliability, productivity, and security. Further, if the quality and safety management standard is implemented properly then no such recommendation takes place during the time of providing Palliative Care. The patient’s goal is also not considered by the respective treatment that is also a drawback of the given care that also can be handled through the respective NSQHS for assignment help.
Further with application of standard 1 of Governance for Health Service Quality and Safety. Palliative care team in the health care sector use governance frameworks to establish, and raise the company's productivity while spreading the word of quality management and the patient experience to all employees. In the workplace, the governance systems are used by clinicians and others. Standards for Effective Governance for Health Security and Improvement require adequate Qualifications for Service Organizations and improvements in Quality and Governance techniques for progress. Now, there are unified regulatory frameworks in place to managing the potential dangers to the health of the patient aggressively. Applying Theory to Practice in the Clinic Care given by the clinical staff is governed by NSQHS of the present day (Quality Health Service, 2022).
Management of performance and competence and leaders and the medical staff possess the
Having the necessary training, experience, and attitude to treatment to Tyler with palliative care is effective and risk-free. In order to enhance security measures, data is analyzed along with Liberties of the Patient and Active Participation. A patient's participation and rights are recognized and helped by being under their care (Quality Health Service, 2022).
Limitations
The most important issue that is related to the chosen standard of NSQHS is partnering with consumers and governance for health and safety lack of knowledge and skills among the service provider that in most cases fail to fulfill the expectations of the patient and also to the family members of the patient in the case of Trajectory Motor neuron disease. Improper infrastructure and incorporation of the family members of the patient is also a big issue and limitation for NSQHS.
Conclusion
Based on the respective case study it can be concluded that Palliative care needs to consider a lot of things and also a particular or more that one standard to provide appropriate relief to the patient not only from the physical pain but also from mental pain. There is not only the consideration of the health of the diseased person that takes place within the respective care by the registered nurse there are also need to include the family members' care. The care that is provided to Tayler was able to support the physical condition of Tayler but no such consideration takes place about his family care. On the other hand there are no such consideration of tools like SAS, PSS, RUG-ADL Score and modified Karnofsky takes place in the care of Tayler by the registered nurse of palliative team, if that is considered with the standard of NSQHS then Tayler must be provided with best palliative care as per the guideline of the Australian Government. The proposed care that takes place with the NSQHs must be provided in the future to the same condition of the person like Tayler it can be hoped.
Referens
.png)
PUBH6003 Health Systems and Economics Case Study Sample
Context
Systems thinking helps us to understand the elements and relationships/interconnectedness of parts to a system. Currently, the use of systems thinking is being advocated in public health as a new paradigm shift. It aids in the solving of complex and intractable public health problems and the identification of risk factors for the achievement of health systems goals/good population health outcomes.
You are required to thoroughly research and write a critical individual report on systems thinking and its application to strengthening the six building blocks of health systems for the reduction/prevention of a chosen public health problem/issue for a selected country.
Instructions
You are required to:
• Identify a country (e.g., Australia or any other country) and a public health issue. Public health problems/issues include excessive alcohol consumption, food safety, heart disease and stroke, road traffic accidents, nutrition, physical activity and obesity, tobacco use, water, sanitation and hygiene, HIV, drug abuse and mental health;
• Provide a critical analysis of the concept of systems thinking and how it can be applied to public health;
• Discuss the six health systems building blocks as proposed by the World Health Organisation (WHO);
• Discuss why the chosen public health issue is complex in the context of the chosen country based on the building blocks and thus requires systems thinking; and
• Apply and analyse how systems thinking can be used to reduce/mitigate the selected public health issue along with the building blocks of the health systems of the chosen country.
Solution
Introduction
Australia is one of the economically stable and developed economies of European Nations, however, the health and infrastructure are considered to be complexed owing to its funding and payment issues. For Assignment Help In the year 2019, 169, 301 deaths were reported within the region of which coronary heart disease was the leading cause in men that is 12% while 12% of females died due to mental health issues like dementia and Alzheimer's (OCHA, 2021). The child death rates were reported to be 76 per 100000 which is lower than in 2009. In addition to this, life expectancy at birth (females) has improved from 1960 which was 74.2 % as compared to 2019 that is 85% (AIHW, 2021a).
In addition to this, life expectancy at birth for males has also improved from 1962 that was 67.9 which has improved to 81. 9% in the year 2019. In recent times, COVID-19 has been the leading cause of death which is 898, however, the disease and incidence rates in Australia have been reducing for the past several years due to which mortality rates have also declined (Australian Bureau Statistics, 2021). The deaths induced by consumption of alcohol reported an upward trend in 2020. The mortality rates during the pandemic were highest with a median age of 86 years with preexisting conditions like dementia, hypertension, cardiac chronic ailments, and hypertension.
Additionally, in the public healthcare units of Australia, the hospital-bed density is 4.0 per 1000 individuals, however, in private houses, there is an average of 4.8 beds for 1000 people (AIHW, 2021b). Also, the Australian public healthcare access is lower or free treatment as costs are majorly covered through Medicare while 46% of the population receives medication from private healthcare units. Besides, the physician density recorded in the year 2015 was 3496 on 1000 population while the population on nursing and midwifery is reported as 12566 on 1000 people.
The chosen healthcare issue is obesity as average Australians are overweight which increases various health risks. More than 70% of Australians are detected with obesity with an underlying chronic health condition that increases the cost of healthcare by more than 30%. Thus, addressing this issue is important for ensuring prevention at an early stage (American Academy of Pediatrics, 2018)
The report will aim at discussing a system thinking approach for addressing obesity as a healthcare problem in Australia.
Obesity as a Healthcare Problem
Concept of System Thinking in Healthcare
System Thinking is referred to as a holistic approach for understanding the interrelation of components, and how each subset operates over a given time frame within larger contexts. In healthcare, it is assumed as a problem-solving approach for evaluating an issue. It analyses the interaction of surrounding elements which greatly impact the problem thus, the evaluation helps understand the entire process for suggesting goals and objectives (WHO, 2010). Thus, in a healthcare context, it is commonly referred to as system-based practice. For instance, for detecting public health issues, system-based practice overviewing individual rehearsal on patients is evaluated within the entire system of healthcare (Brennan, Kumanyika&Zambrana, 2014). Thus, it aims in making healthcare successful by undertaking goals for individual patient levels. However, many diseases like obesity have not been addressed appropriately through system-based practice due to the population with existing conditions coupled with overweight has been increasing for years.
Six Building Blocks proposed by WHO
Service Delivery- Service delivery is commonly assumed as the output of all resources used for making the healthcare system efficient. It might include workforce, supplies, finances, and others. Thus, for improving the outcomes, it is important for aligning the inputs in a way for enhancing the overall service delivery models (WHO, 2010)
The service delivery for providing healthcare resources to treat and prevent obesity includes in-patient and outpatient services. The hospitals face the struggle of huge managing patient counts which impacts early intervention strategies. However, several local governments like NSW have devised strategies like obtaining free health coaching through calls on toll-free numbers which helps individuals in receiving assistance on health goals.Dietitians Association of Australia is also created for publishing campaigns and devise strategies for controlling weight and supervising health-related objectives. However, the Australian Healthcare system has been facing issues like increasing costs, experience for the patients, accessible points of care which have impacted service delivery due to which obesity is considered to be one of the crucial healthcare issues from the past few decades (Clarke et al., 2021).
Healthcare Workforce - The capability of nations like Australia for meeting health goals relies largely on knowledge, motivation, and skills. There is a direct link between the health workforce and the health outcomes of the entire population (WHO, 2010). Australian Healthcare Industry has been facing acute healthcare shortages thus reducing capabilities for meeting the increasing demands from aged care and child care. It is estimated that by 2015, there will be a shortage of approximately 1000000 nurses in inpatient and outpatient services for managing the underlying condition of chronic disease like obesity.
Health Information System- WHO defines that every healthcare organization is only successful if it has reliable data for making an efficient decision. The health information system is highly dependent on the main key factors that are the generation of data, compilation, synthesis, and communication of information to vital stakeholders (WHO, 2010). Australian Healthcare is on the stage of technical transformation with digital strategies proposed by the government, although the application of technology is at infant to mature stage which poses issues in treatment and flow of information from service providers to insurance companies.
Accessing essential medicines- A health care system that is characterized as well functioning ensures that the population receives equitable medicines, vaccines, and other healthcare resources with approved quality, costs, and efficiency (WHO, 2010). For achieving equitable supply of medicines and other healthcare resources, national healthcare policies, guidelines, trade practices, pricing strategies must be effectively aligned with healthcare goals. Australian Healthcare system has an efficient supply of generic and specialty medication, although indigenous populations are provided medication through the community sellers for improving life expectancies.
Financing of Health system- Finances holds a crucial place for ensuring the efficacy of healthcare resources. If necessary, funds are not allocated then workforces would not be employed, no medicines will be supplied while the entire functioning of the healthcare system will be paralyzed (WHO, 2010). The financing healthcare system is dependent on two objectives that are for raising sufficient funds and providing financial risk protection to the entire population. Major issues of healthcarein funding from local and state governments. Also, Medicare increases the complexity of healthcare outcomes as payments are delayed due to a lack of transparency and efficient flow of information in treating chronic ailments like obesity.
Leadership and governance- Leadership and governance ensure the existence of a strategic policy framework that is combined with coalition, regulation, addressing system design, and accountabilities. As per WHO accountability is one of an intrinsic part of leadership and governance as it relates to balancing & managing relationships amongst the population, governmental organizations, non-governmental organizations, households, and other entities (WHO, 2010). Leadership gaps are quite prevalent at every stage of governance which has impacted efficient utilization of resources that has patient outcomes for people with obesity.
Barriers for Applying System Thinking Approach
The system Thinking approach includes the integration of elements for understanding the core issues. Australian Healthcare industry has been witnessing an increase in obesity rates in younger as well older populations. Thus, the system lacks implementation, integration, and evaluation of public health strategies at the community level. One of the profound steps taken by the Australian Government includes banning fast-food advertisement in prime time accompanied by restrictions on retail sectors for selling, promotion, and display of sugary drinks. Lack of uniform monitoring and supervision of meals served in schools and college canteens is one of the implementation issues which is owned barrier of leadership and funding. It is observed that the younger population has a greater inclination to barging on sports drinks, cheesy items, and other foods with trans fat (Clarke et al., 2021). The complex healthcare model accompanied by workforce shortage has increased obesity and related conditions. Technology can be a great facilitator for improving system thinking, although building IT infrastructure requires substantial investment due to which digital strategies have been delayed. Also, privacy and security-related issues have been increasing in past years that have impacted the larger implementation of digital tools for managing service delivery and patient outcomes.
Recommendations for Improving System Thinking
Australian Healthcare system is recommended for prioritizing whole food consumption policies accompanied with physical activities in school and colleges. Also, healthcare practices and campaigns that promote water and vegetable consumption must be introduced. The healthcare leaders are suggested for engaging the wider communities for meeting malnourishment targets while initiatives must be undertaken for improving food environment at school.
Conclusion
Obesity has emerged as one of the chronic health problems of Australia, thus, six building blocks by WHO have been used for identifying issues in detail. System-based approaches lack health policies for managing obesity. Thus, leaders need to collaborate with different stakeholders for applying a system thinking approach to improve the health and well-being of the Australian population.
References
.png)
PUBH6000 Social Determinants of Health Case Study Sample
Context
The social determinants of health play a major role toward disease, health and wellbeing of the community. This assessment is aimed at consolidating students understanding of how the social determinants of health affect the health outcomes of a population. The assessment gives you an opportunity to demonstrate your understanding of the fundamentals of public health practice and apply theoretical and conceptual health intervention frameworks to analyse the health of a population. This assessment task is also designed to further develop your ability to reflect on your practice. As a public health practitioner, it is important to develop your ability to reflect on personal experiences, feedback and assess your own capabilities. This practice of reflexivity supports personal and professional growth.
Task Summary
In this assessment you are required to read a case scenario provided by your Learning Facilitator, using critical thinking skills develop a report demonstrating your ability to apply theory into practice. Your report should be 1500 words (+/- 10%) in length. In addition to submitting assessment 2 Part A, you are required to provide another 200 words of learning journal demonstrating your ability to reflect on personal experiences and challenges working to complete Assessment 2 Part A . Use the assessment template provided to develop this assessment.
The scenario will be provided separately.
Please refer to the Instructions for details on how to complete this task.
Instructions
1. Read carefully over the given scenario provided by your Learning Facilitator.
2. Research health issues and relevant social determinants of health that would influence health outcomes of the population in the given scenario
3. Use the Ecological Model to analyse factors relevant to the scenario that influence health behaviours and health outcomes of the population in the following perspectives.
• Intrapersonal level
• Interpersonal level
• Community level
4. Reflect on your thoughts/activities and challenges in preparing the assessment in the Learning Journal such as information provided to complete the assessment, class activities, searches for further information and references.
Solution
Introduction
The key focus of the assignment is on the disability system in Australia and the impact of relevant social determinants on the health outcome of the Australian population. Accourding to The Assignment Helpline, The case study of a disabled Leo has been used to refer to the various challenges disabled people in Australia might go through although the theoretical perspective is mostly generalized health system. The ecological model consisting of intrapersonal, interpersonal and community level factors have been used to determine the influence on health behaviours and health outcomes. Reflective summary of the experience regarding the assignment has also been provided as learning journal at the end.
Context of Potential Health Issue Among The Population
The survey report of Disability, Ageing and Carers in 2009 revealed that 18.5% of the Australian population or about 4 million people are disabled. In addition to this, another 21% is affected by long-term health condition but is not restricted from everyday activities. 87% of the people with reported disability suffer from specific limitation that restricts them from performing mobility, communication and self-care activities("About People with Disability in Australia | Department of Social Services, Australian Government", 2021). Although there are other health issues that is covered under the entire healthcare system of Australia, the key focus in the case study scenario is disabled people with Leo being one of them. It is quite difficult to define disability but from a general perspective it can be referred to the condition that can hinder a person from their ability to carry out day to day activities (Emerson & Hatton, 2014). However, there are varied degrees to which the disability can hinder a person ranging from mild like needing to wear reading glasses to severe where there is brain injury. According to the Report on Government Services 2002 the three core activities that form the basis of disability includes self-care, mobility and communication. Based on these activities, the ABS Survey of Disability, Ageing and Carers defines 4 levels of disability namely mild, moderate, severe and profound.
There are several issues that people with disabilities have to face and are more likely to experience than people without any disability. Issues like social isolation and fewer opportunities to participate in community life are more probable for disabled people ("Face the facts: Disability Rights | Australian Human Rights Commission", 2021). Moreover, such people are also more subject to living in poor quality, experience poverty, acquire low levels of education and obtain insecure housing. Studies show that some of the greatest causes of disability include mental illness and mental health problems which also diminishes their quality of life and reduce productivity levels. In the Australian population, workforce participation of disabled people is only 54% as compared to 83% of non-disable people ("Disability Support and Services in Australia – Parliament of Australia", 2021). Also, among the OECD countries, Australia has the lowest rank for the relative income of disabled people. Although the Australian government has planned on making all public transport accessible to disable people by 2022, reports show that about 1.2 million disabled people are still struggling to use them properly ("About People with Disability in Australia | Department of Social Services, Australian Government", 2021). Young people with disabilities like cognitive impairment in Australia are six times likely to end up in prison as compared to their non-disable counterpart. On the other hand, 90% of women with intellectual disabilities are subject to sexual abuse where more than a quarter of all disabled people are sexually assaulted in Australia("About People with Disability in Australia | Department of Social Services, Australian Government", 2021).
Social Determinants of Health
The social determinants of health issue refer to the disadvantages that contribute to their poor health and disabled people and their carers are the most disadvantageous group in Australia. The ecological model has been used for critical analysis of the multiple levels of influence on health behaviours of the disabled people in Australia. These include intrapersonal or individual factors, interpersonal factors and community factors ("Ecological Models - Rural Health Promotion and Disease Prevention Toolkit", 2021).
Intrapersonal/ Individual Factors:
The intrapersonal factors influence behaviour such as personality, beliefs, knowledge and attitude and are directly impactful on the individual with the disability. The social determinant that impact on an intrapersonal level is education. The more people participate in the workforce, they acquire higher levels of education and as a result of this achieve better health. Regardless of the impairment types, people with disability have on average lower levels of education as compared to other non-disabled population. Only 24% of the disabled people have completed year 12 or equivalent in terms of educational qualification which quite low than non-disabled people with 46% completing the same educational level ("Social Determinants of Health - Integrated care", 2021).
The National Disability Insurance Scheme (NDIS) provided support through local provider in town for Leo as part of their mission “no one is left behind” which includes 430,000 disabled Australians ("Social Determinants of Health - Integrated care", 2021). Leo lived on his own with the help of the services received from the local provider and was meant to be learning skills that help him live a more independent life. However, the behavioural concerns and continence issues prevented Leo from acquiring the learning skills which has impacted him on an intrapersonal level.
Interpersonal Factors:
The interpersonal factors include social support acquired from interaction with other people or create limitations in enhancing interpersonal growth that can lead to healthy behaviour. Employment can be considered as such a factor that offers opportunity for social support. Both people with disabilities and their carers have lower employment levels which lead to lower incomes and higher rates of poverty. In addition to this, enrolling in the workforce also involve social inclusion, decision-making and autonomy for the disabled person. Disabled people in Australia are almost 50% less likely to be employed which is also well below the OECD recommended 60% (Carey et al., 2017). Even more, disabled women are less likely to be in the workforce as compared to men which further limits their chances of social inclusion.
In the case study, as Leo received services from the NDIS, he lived on his own but was still unemployed as he failed to acquire the learning skills. Moreover, the notice from the service provider to cease all support further worsened the long-standing behavioural and incontinence issues of Leo and his family was quite insecure about his future. It was the complex disability of Leo affecting his cognition, emotional regulation and ability to perform daily task that prevented him from getting employed in the first place.
Community Factors:
These factors include the formal and informal social norms that can limit or enhance healthy behaviours of disabled people through interaction among individuals, groups and organizations. Housing is one such factor and is also linked to health of the disabled individual. Affordable, secure and suitable housing for the disabled is rarely available which makes them vulnerable in the Australian housing market. Instead of residing in cared accommodation establishments, almost 95% of disabled people in Australia live in regular households ("Social determinants of health - Australian Institute of Health and Welfare", 2021). As a result of this, people with disability might often fall out of home ownership and become rental tenants.
The reason the chief executive of Leo’s provider stated of withdrawing the services is the unhygienic condition due to the mess made by Leo. This was considered as an unacceptable risk for everyone and might also compromise the safety and well-being of Leo and the staff members. However, as Leo was suffering from continence issues, a regular household instead of cared accommodation would result in such mess and unhygienic conditions.
Influence of The Key Determinants on Health Behaviours and Health Outcomes
The social determinants from all three levels of the ecological model influence the health behaviours and health outcomes of the disable Australian populace. The lowered rate of employment leads to lower income and increased poverty for the disabled people. As compared to other OECD countries, Australian disabled people live in much worse conditions. As a result of this, the median personal income for disabled people was $225 per week while the non-disabled people had $480 ("SHUT OUT: The Experience of People with Disabilities and their Families in Australia | Department of Social Services, Australian Government", 2021). The intrapersonal factor of education is also linked to this outcome as there is existing income inequality for disabled people regardless of their educational qualification. The higher poverty rates in turn make it eve harder for disabled people to acquire care services which affects them on a community level as well. For this reason, government backed general resources, support and services provided by NDIS helps disabled people overcome the health outcomes caused by the key social determinants (Kavanagh, 2020). Disabled people like Leo and others can live an independent life on their own without worrying about employment and income.
Conclusion
It is evident from the assignment that as compared to other OECD nations, Australia currently is ranked lower in terms of services provided as well as well-being of the disabled people. The critically discussed social determinants from all three levels of the ecological model indicate that Australian population of disabled people are far more likely to suffer from unemployment, poverty and homelessness as compared to non-disabled populace.
Learning Journal
References
.png)
MBA623 Healthcare Management Case Study Sample
Your task
Individually, you are required to write a 2000-word analysis based on the annual report provided in MyKBS, under the assessments tab.
Assessment Description
In this assessment, students will be given an opportunity to analyse the environment of healthcare management in Australia and the increasing need to deliver better value to all stakeholders by applying the principles of best practice leadership, team-building and organisational design in a healthcare setting. You will need to demonstrate an understanding of the policy framework and the system dynamics driving change in the healthcare sector and an ability to evaluate the importance of sound financial management for healthcare organisations.
Assessment Instructions
An important skill that a healthcare manager must develop is the ability to analyse a health service or organisation in terms of how well it is meeting its stated mission and objectives. Using the information from the Annual Report that will be provided to you in electronic format, you are to write a formal report that investigates the central organisation in terms of its:
1. Political and policy environment
2. Organisational design and coordination
3. Leadership and teamwork
4. Financial resource utilisation
5. Attitude to, and utilisation of, technology
From your analysis of these elements, you will attempt to identify areas where improvements may be sought. You will justify your arguments for why these improvements should be introduced and present them in the form of detailed recommendations to the Chief Executive and the Board. You will undertake whatever additional research is required to give you a better understanding of the organisation and its activities and any research that is needed for you to formulate your recommendations. This research will form the basis of the Reference List of your report. The primary sources for research should be relevant published academic journals and texts but other sources of information such as newspapers, magazines and reports may also be of value. As stated earlier, the format for this assessment is a formal report. If you have not undertaken a task like this before, your research would also include how to structure and present information in a report format. An Executive Summary is considered to be a key component of a formal report and in this instance is included in the word count for this assessment.
Solution
Political and Policy Environment
The political stability in Australia is quite good, as the organisations operating in different industries including the healthcare sector are provided with proper support and resources to establish the overall healthcare segment in the country. For Assignment Help, The legal acts imposed by the political organisations emphasise on the healthcare development all across the country, and on the grounds of this organisations such as Calvary set up their internal policies integrating them in their SOPs (Standard Operating Procedures). Calvary Health Care Bethlehem continues to adhere with the policies imposed by the government on the basis on competitive neutrality. The organisation revised its healthcare policy of being culturally responsive towards the Aboriginal and Torres Strait Islander Community by leading on to a new direction acknowledging the policies of government (Calvary Health Care Bethlehem, 2021). Since 2019 August, an important body of work has been initiated and carried out in order to screen for the cognition alterations alongside the delirium on the ward. The execution was directed by a new policy alongside a program of education and learning. The ongoing screening education for the new medical workers has been integrated in their orientation program and the results concerning the same are presented regularly during the meeting with medical staffs (Dixit and Sambasivan, 2018). Apart from this, the significant accounting policies of the organisation comprise of taxation policy, goods and services tax, income recognition, and revenue recognition policy. All these policies are accounted when preparing the financial report. Out of these, the key changes in company’s accounting policy relates to the timing of the revenue recognition from applying the AASB 15 under different streams of revenue. The auditing group evaluate the appropriateness of the all these policies used by the organisation alongside its reasonableness comprising of the accounting projections, as well as related disclosures made the board of directors (Calvary Health Care Bethlehem, 2021). However, there are certain policies concerning the welfare of the public that are not adopted as of now, but might turn out to be an essential policy in the future.
Organisational Design and Coordination
In an organisation such a Calvary Health Care Bethlehem, it is of paramount importance to have a proper strategy in place concerning organisational design and coordination. The efficient functioning of a health service is influenced by the organisational structures alongside the coordination. The organisation structure of Calvary Health Care Bethlehem comprises of arrangements including responsibilities, authority, information and knowledge sharing, and result. The organisational design of Calvary Health Care Bethlehem is a formal and directed process used for incorporating people, technologies, and information (Calvary Health Care Bethlehem, 2021). This serves as a key structural component, which makes it feasible for the organisation in maximising the value through aligning their hierarchical design with the overall vision and mission of the company. In a healthcare setup such as Calvary Health Care Bethlehem, the importance of coordination among the different departments needs to be quite high and effective, as it is directly related to the outcome of a patient. It is of utmost importance for the healthcare managers to ensure smooth and hassle-free coordination in order to reap fruitful results by providing a thorough treatment to their patients.
At the micro-level of Calvary Health Care Bethlehem, medical professionals are grouped together in order to work in units having a mutual supervisor. The structure of any organisation is quite complex by nature, and there is a high possibility of problems taking place every now and then accompanying the company benefits indirectly (Sandhu, 2019). Every company design has certain dysfunctional as well as functional characteristics. As per the structural contingency theory, it is of importance to consider the complex trade-offs within the design of organisation. Integration and differentiation are two vital components in this case. Integration includes the coordination of activities between the healthcare units, comprising of conflict management resulting in better patient outcomes (Heath et al., 2017). On the other hand, in differentiation every part of the company is managed in order to meet a specific need of speciality work in the healthcare setup. From the application of this theory in Calvary Health Care Bethlehem, it can be stated that the organisation somewhat adopts and follows a hybrid approach to carry out their operations. Although it is of extreme importance for Calvary Health Care Bethlehem to have their total focus on better patient outcomes, which they do, but in certain instances, the organisation also needs to use the differentiation approach in order to meet a specific need of a specific group of patients (Calvary Health Care Bethlehem, 2021).
At the macro-level of Calvary Health Care Bethlehem, there is a significant interdependence accounting for interconnectedness of work, task uncertainty, size, sharing of resources, and so on. Thus, the organisation needs to have a structural approach in place for ensuring a smooth coordination concerning the hierarchy, procedures and rules, planning and objective setting, lateral relations, and vertical information system. In this context, the organisation makes use of a program organisation design. In this design, the organisation standardises the work processes by using rules, regulations, plans, schedules, policies, procedures, and protocols. This design also allows the organisation in standardisation of skills with specification of skills or training needed to carry out the work, as well as standardisation of output by specifying the form of intermediate outcomes of work (Ali et al., 2017).
Leadership and Teamwork
Leadership is a vital aspect for any organisation operating in any industry. In this context, leaders entail the frontline managers directly supervising the care providers, middle managers accountable for their respective departments, and the top managers such as CEO for managing the entire organisation (Fletcher et al., 2019). The leaders of Calvary Health Care Bethlehemfocus of strategic way of solving issues by incorporating strategic function in their leadership constituting of objectives with subsequent action for achieving the same. As known, the internal system of any healthcare organisation involves numerous complexities giving rise of problems. The 8-step strategic problem-solving process can be used, as it provides an integrated perspective towards a problem resolution, and can provide fruitful results. Besides this, the leaders of Calvary Health Care Bethlehem adopt a transformational leadership skill, as for implementing a certain change needs clinical and administrative leadership (Calvary Health Care Bethlehem, 2021). Alongside this, sustaining the leadership in Calvary Health Care Bethlehem is also quite effective, as they have a proper strategy in place for succession planning and self-care. The members of Calvary Health Care Bethlehem are highly motivated for the upcoming initiatives being brought to the table for development of better care for the patients. Furthermore, the members with managerial roles in the organisation are clinical with communication, as for making a team to get a job done efficiently it is imperative. It is often seen that due to lack of communication between the speciality groups led to unfortunate outcomes for the patient.
Moreover, teamwork is another essential component in Calvary Health Care Bethlehem led by leaders will excellent leadership skills. The teams and units working with each other provided with a defined purpose, composition, structure, and specific processes. The teams work as a formal group within the organisation, which is task-oriented with a specific purpose. The teams operate staying in the organisational context and interact with organisational sub units to ensure proper medication of the patients. The work teams of the organisation collaborate for providing a specific service, the support teams provide support for the primary functions, the parallel teams include individuals serving within the work teams also play a vital role in assisting, the project teams produce one-time outputs, and management teams provide the overall direction having a purpose (Sfantou et al., 2017). All these departments conducting a set of activities hold a value for the stakeholders including themselves, as well as the patients, their family, other associated medical firms, and so on.
Financial Resource Utilisation
The Australian government spent an amount of 185 AUD on the health services and goods during 2017-2018 (Calvary Health Care Bethlehem, 2021). However, the real financial problem existing is that the mix of funding alongside the responsibility of the service delivery amid the state or territory governments and the commonwealth. This discrepancy has led to shifting of costs and gross inefficiencies, alongside poor service integration. As per the financial reports of Calvary Health Care Bethlehem, it can be said that the organisation has a well-managed flow of financial resources with apt use for treating their patients with utmost care and medication (Edney et al., 2018). The rise of globalisation has influenced the overall healthcare sector due to which the organisation was required to make use of their financial resources not only for people of Australia, but also tying up with healthcare institutions in other countries to create a positive relation, which can pay off during the need of the moment. Besides, it has been identified that some of the medical expenses this company receives from funding from the Victorian department of health due to its name in the denominational hospital list. It is a great help in managing both time and financial resources.
Attitude To and Utilisation of Technology
Calvary Health Care Bethlehem each year works on interdisciplinary teams for collaborating them for developing the assistive technology resources for improving patient quality of life. Current important updates involve developing modified eye gazing systems, interaction processes as well as environmental management teams for patients’ wheelchairs. New planning devices have additionally brought to enable patients for driving wheelchairs along with management of other devices through a single change during hand movements are impaired. Change management options have developed patients’ skills for using mainstream technologies like iPADS, mobile phones, and tables. Permission to these devices on wheelchairs permitted effective selections and management over how they interact, move and work relaxingly (Poojitha, 2018).
The Vitro application has been applied in Calvary Health Care Bethlehem in 6 months end-to-end offering the healthcare company with an entirely paperless process in which all medical information was being stored electronically. This project unit that involved all medical employees from both the Calvary Health Care Bethlehem team and Vitro group have worked collaboratively for identifying as well as reviewing the present paper forms of that total 197. At the time of reviewing procedure this became evident that streamlining as well as effectiveness can be made, the opportunities was taken to evaluate the needs of Calvary Health Care Bethlehem that outcomes in the minimization to 67 forms that would be converted in Vitro applications.
Recommendations for Improvements
Focus on better technologies should be one of the current solutions for Calvary Health Care Bethlehem as well as overall healthcare industry in 2021. Applying the online data as well as modern interaction tools efficiently will be needed for the future of the care unit in Calvary Health Care Bethlehem. Technology will act as a role in around each area of health, involving health record keeping. It can be said that developing an online health recording process in Calvary Health Care Bethlehem similar to My Heath Record. Having this type of portal and record keeping app will help the company in providing and accessing major health data of all the patients (both old and new) involving any past allergies, health conditions as well as treatments, medicine history along with scanning reports can be evaluated by one system in the entire Calvary Health Care Bethlehem. On the other hand, it can be said that this type of change in the company will also help the medical practitioners, doctors, health care workers in this company working in remote, regional areas. Online technology will ensure this probable for the medical care workers and doctors in Calvary Health Care Bethlehem to have video appointments with all the patients who cannot visit to the centres or Calvary Health Care Bethlehem hospital for appointment with experts. This type of solution is particularly relevant and impact in the current COVID-19 pandemic.
Reference List
.png)
CAP203 Care of The Person with an Acute Illness Case Study Sample
Assessment Task
This assessment is designed to further assess your knowledge of pre-operative nursing care. This assessment follows on from Assessment 1. From your analysis of the case study you will answer a series of questions. Please refer to the Task Instructions for details on how to complete this task.
Context
The Registered Nurse plays an important role in the preparation of a person for surgery. This assessment provides you with the opportunity to apply theory to a clinical scenario. To complete this assessment you will need to apply clinical reasoning processes as you continue to examine the case study from Assessment 1.
You will be required to integrate the information from analysis of the data provided together with your knowledge of pathophysiology, clinical manifestations and legal and ethical principles to the holistic nursing care of a person during the pre-operative period of an acute surgical admission.
You will need to use the following processes from the clinical reasoning cycle to complete the assessment:
- Establish Goals
- Take action
Instructions
To complete this assessment, you will need to examine and analyse the case study presented below and provide responses to the questions asked.
This assessment continues on from Assessment 1 and now requires you to identify the appropriate nursing interventions and specific goals required for the patient problems identified in Assessment 1.
The case study is provided below for your further analysis.
Case study
Maria Romano is a 76 year old woman admitted to the Emergency Department via ambulance. Maria fell when watering her garden and was unable to get up. She was lying in her garden for 3 hours until her daughter came home from work and found her. Maria's medical history includes osteoporosis, glaucoma and she has recently been diagnosed with early dementia. She has no significant surgical history. Maria lives with her daughter Paulina and Paulina's husband, Sam. Maria's current medications include Aspirin 75mgs daily, Alendronate Sodium 10mg orally daily & Latanoprost eye drops to both eyes nocte. She was administered Intravenous Morphine and inhaled Methoxyflurane by the paramedics.
Assessment data:
Airway: patent
Respiratory rate: 18 breaths/min Oxygen saturation: 97% on room air Heart rate: 90 beats/min Blood pressure: 110/70 mmHg Capillary refill: 2 seconds
Right leg shortened and externally rotated Right hip bruised and oedematous
Right foot pink, cool to touch, no paraesthesia or abnormal sensation, pedal pulse present
Alert: orientated to time and place Pain score: 5/10 on rest, 7/10 on movement
Temperature: 35 C
Small laceration to lower left leg
Blood glucose: 9 mmol/L
Intravenous cannula inserted Cephalic vein Left arm
X-rays reveal an Intertrochanteric fracture of the Right femur. Maria is seen by the Orthopaedic surgeon and is scheduled for an Open Reduction and Internal fixation (ORIF) of the fracture. She has been placed on the Emergency Operating List. The Registered Nurse has just administered Intravenous Morphine 2mg and the anaesthetist has been contacted to perform a femoral nerve block. The orthopaedic registrar will visit Maria in the next 10 minutes to gain consent for the surgery. Maria is accompanied by Paulina, who is clearly upset about her mother's hospitalisation. Paulina informs you that she is so worried about how thin Maria is.
She is also concerned that Maria has been falling frequently over the past few months, she purchased a walking frame for Maria but she rarely uses it. You note that Maria is upset that she is going to require surgery. She is worried about her garden and who will water it while she is in hospital.
Questions
- Discuss the Registered Nurse's role regarding the issues related to informed surgical consent, confidentiality and privacy that were identified in Assessment 1 (120 words)
- Develop four short term goals to be achieved in the pre-operative period. These goals should relate to the problems identified in Assessment 1. Discuss who must be involved in the development of these goals (80 words)*
- Discuss the nursing interventions required to meet the identified goals and pre-operative patient problems (from Assessment 1). Ensure that rationales are provided for these interventions (400 words)*
- Answers to Questions 2 & 3 can be presented in a table (see a suggested format below)
.png)
Solution
Registered nurses’ role
In the case of Maria, consent issues arise in terms of accompanying her immediate family, her daughter Paulina, in the surgical process and recovery from her current cognitive condition. For Assignment Help, Maria's current cognitive condition interim of dementia has made informed consent difficult, and her daughter Paulina is also upset about the hospitalisation; thus, there is needed to manage the situation for informed consent. As per Australian healthcare guidelines, informed consent is taken only after giving accurate and relevant information regarding intervention and outcome, as well as ensuring privacy and confidentiality to the individual (Australian Commission on Safety and Quality in healthcare, 2022). The role of the RN here is to delegate and provision the informed consent process and ensure that the patient and immediate family has enough knowledge of the process to give informed consent (Queensland Government, 2022). Also, maintaining privacy and confidentiality related to patient’s problem help in the healing of the problem quickly. Similarly, in the case of Maria, the RN has to follow the same.
Short term goals
- Providing energy to the body
- Increasing haemoglobin in the body before surgery
- Managing pain associated with fracture
- Assuring Maria to avoid preoperative distress
While developing the goals, surgeons, orthopaedics, nutritionists, general physician as well as registered nurses are needed to be involved.
Nursing intervention
.png)
.png)
.png)
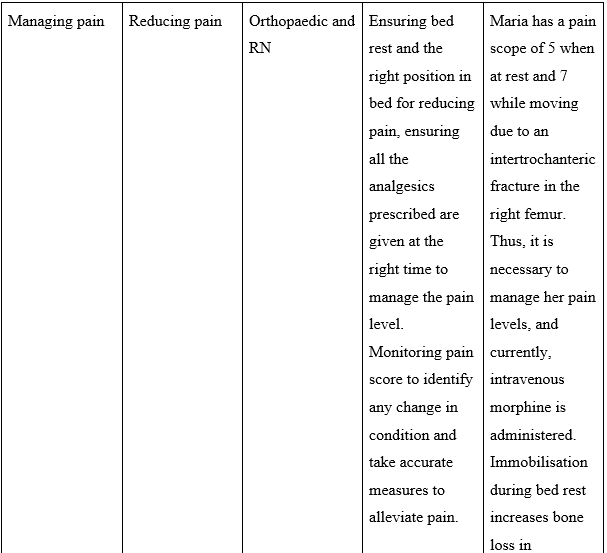
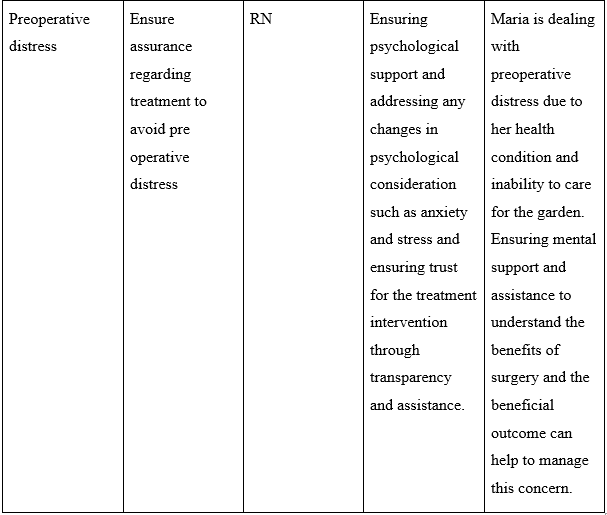
References
.png)
LMED28001 Chemical Pathology Case Study 1 Sample
The total word count for this case study report is between 2,000 to 2,500 words (excluding references). Reports should be typed in Word and adhere to the format of the given template (Arial, 12pt, Single spacing).
The report must be your own work and your name, student ID and page numbers should be included in the footer of all pages of the report.
Abstract: 10 marks (200 words max)
Criteria for High Distinction in this section:
The abstract should provide a clear and concise overview of your report and the findings of your biochemical tests. A clear but brief outline the case history is provided, along with the tests performed, rationale of the tests and how they can be used to diagnose the specific disease to reach a final conclusion in this case.
No references are included in the abstract.
Introduction: 15 marks (400 words max)
Criteria for High Distinction in this section:
The introduction should clearly outline the necessary background information, including signs or symptoms, underlying pathophysiology, clinical and the laboratory information of relevance.
A clear and concise explanation of aims and objectives of the tests are provided, with a brief conclusion to the section specifying the conclusion/diagnosis with no discussion.
Materials and Methods: 10 marks (no word limit)
Criteria for High Distinction in this section:
The methods that you have used or intend to use (further tests) to arrive at the provisional diagnosis are clearly and concisely summarised.
The sources to these methods need to be clearly referenced, even if it is simply the prescribed text/lecture material/laboratory manual. Reference is made to specific instrumentation that could be used to conduct these biochemical tests (e.g. biochemistry analyser) and the manual is sufficiently referenced. The written work is an original and brief summary of the method used and not a reproduction of text from these references.
Results: 20 marks (no word limit)
Criteria for High Distinction in this section:
The results section provides a clear summary of all data/results with reference ranges.
The layout is clear, legible and uncluttered. All figures or tables are labelled clearly with legends where appropriate. Units have been properly included.
Interpretation of results is limited to a description of how they compare to the normal reference ranges. The results are presented, however not discussed in this section. Further tests (if required) with expected results are outlined.
Discussion: 30 marks (No word limit)
Criteria for High Distinction in this section:
Provisional and differential diagnoses (if any) should be clearly stated and discussed with reasons provided in relation to the clinical and laboratory results.
Expected results of further tests must be included to support your provisional diagnosis and/or align with your differential diagnosis(es). Your conclusions reached and the evidence required to reach these conclusions is compared with existing literature on similar case studies.
The full text of the published articles forms the basis for this discussion (don’t draw comparisons from other abstracts without reviewing the full text of the articles). The pathophysiology of the diagnosis and possible treatment options (if any) are also discussed. Finish your discussion with a final concluding statement.
Solution
Abstract:
The report has been carried out focusing on the case study of an 80-year-old man who was admitted to the ER due to certain signs and symptoms which included chest pain, shortness of breath, and severe cough. After admission to the er the patient was provided with blood tests or serum biochemistry assessment where certain proteins and enzymes were evaluated in order to assess any underlying abnormality It was found that the patient sustained abnormality in anion gap, urea level as well as creatinine level. For Assignment Help, Based on these abnormalities the patient was provided with three diagnostic tests which included UEC tests, troponin test as well as CK-MB test. Each test was carried out based on their respective field of assessment as the UEC test was provided to evaluate urea level electrolyte level as well as creatinine level in the Serum. Further CK-MB test was carried out to evaluate any suspected risk of heart attack and a troponin test to analyze any threat of renal failure or cardiac muscle damage. After completion of the assessment of the selected three biochemical tests, it was found that the UEC test along with the anion gap test provided better insight into the underlying health condition. The biochemical test assessment highlighted the risk of renal failure in the patient which led to the state of shortness of breath, chest pain, and cough.
Introduction:
The report focuses on analyzing and evaluating the case study of a patient named Mr. David Gilmour who is 80 years old and was admitted to the ER Department of a local hospital. The patient was admitted with a major complaint of chest pain Cough as well as difficulty in breathing. After admission to the er blood Cup squad was conducted in order to analyze the vitals of the patient after 24 hours of the blood test a second work was initiated in order to sustain detailed information post admission to the ER and provided healthcare assistance. It has often been found that heart failure often leads the heart muscle towards deprived pumping of blood. In such conditions, fluid built up occurs within the lungs which causes shortness of breath in the suffering patient. Similarly in the case of renal failure, often flute retention in the lungs leads to chest pain and shortness of breath which were two of the main symptoms identified in the patient. It has also been found that often chronic kidney disease or anal failure leads to a heart attack as the heart withstands increased pumping of blood to deliver it to the kidney.
On analysis of the serum biochemistry of the patient, it was found that on Day One the anion gap counts 5 which was the same on the day to result. It was also found that the urea and creatinine levels also increased from their normal reference ranges. The urea level in the serum was 18.9 on day 1 and 17.5 on day 2 at the same time creatinine level was 0.18 and 0.16 on the respective day results. After evaluation of the blood test on Day 1 and Day 2, three tests were requested for the patient in order to identify and evaluate the underlying causeway of the signs due to which the patient was admitted to the ER. The tests include blood UEC, CK – MB, and proponent test which are used in order to suspect myocardial infarction for heart attack sustained by the patient. These tests are used in order to evaluate the risk of heart attack and kidney function in relation to abnormal Creatinine, Troponin as well as Urea levels in the Serum. The report does will focus on analyzing and evaluating the two chief suspected underlying health conditions; heart attack and renal failure with the use of 3 referred biochemical tests.
Materials and Methods:
Blood – UEC
UEC test is also known as the kidney function test but just carried out using the assessment of urea, electrolytes such as potassium, sodium, and chloride as well as creatinine. Electrolytes and urea are accounted to be the most frequently used biochemistry test which helps in the assessment of Renault failure or associated kidney health (Dhanani et al., 2018). Urea and electrolyte tests provide significant information in terms of hemostasis and excretion and the inclusion of a creatinine test supports the result with glomerular filtration rate within a patient (Bamanikar, Bamanikar & Arora, 2016). In order to conduct advanced electrolyte tests, often Anion Gap Blood Test is carried out in order to evaluate the acid-base balance or PH balance of a patient’s blood. This test indicates whether the blood is acidic or non-acidic in nature based on the electrically charged minerals present in the body which includes bicarbonate sodium and potassium (Yang et al., 2017).
CK-MB Test
The CK-MB test is a standard blood test that is used to analyze and measure certain enzymes released in the blood first of these enzymes includes the creatine kinase-myocardial band. This enzyme is generally released from the heart when the heart or muscle from other parts of the body sustains severe damage. Generally, creatine kinase is present in the heart but it releases creatine kinase-myocardial band after muscle damage (Kim & Hashim, 2016). It has also been found that in the case of renal failure, the creatine kinase-myocardial band is falsely elevated due to muscle damage in the kidney. ichroma™ CK-MB is known to be a fluorescent immune assay or FIA which is used as a diagnostic procedure for Creatine Kinase Isoenzyme-MB in the blood or serum of the human body (Lab Industries, 2016).
Cardiac Troponin Test
Cardiac troponin tests are used in order to measure the troponin T or troponin I protein level in the blood. It is used in order to assess heart attack or suspected renal failure as Troponin proteins are released in conditions where the heart muscle sustains damage. The test indicates the amount of damage that occurred within the heart as the greater the amount of released troponin proteins in the blood, the greater the damage cardiac-specific troponin biomarkers are generally used in relation to different symptoms along with abnormal ECG as well as suspected myocardial infarction in case of patients suffering from chronic kidney disorder (Mair et al., 2018). Cardiac Troponin assessment is carried out with the help of standard blood tests where blood samples are used in order to measure the amount of troponin raised in the blood.
Results:
In the case of a creatinine urine test, urine samples are corrected over a period of 24 hours in order to assess the creatinine released out of the body. The normal range of Serum creatinine is 0.04 – 0.12 mmol/L which when exceeds indicates an abnormality in kidney function or renal health (Delanaye, Cavalier & Pottel, 2017). The electrolyte test examines the sodium, manganese, and potassium level in the blood which actively maintains the acidic and nonacidic nature of the blood. It is also used in anion gap blood tests which helps in evaluating the pH of the blood. An increase or decrease in anion level or electrolyte level in blood leads to shortness of breath and heart attack. The condition was similar in the case of the patient as the anion gap was 5 which was below the normal range of 10 – 20 mmol/L. The urea test indicates the normal ability of the kidney to break down urea, of the level of urea in the blood is high then it indicates kidney failure or renal disease. The normal range of urea in serum is 2.5 – 8.6 mmol/L, but in the case of the patient, the range was 18.9 and 17.5 within a period of 24 hours indicating abnormality (Laville et al., 2023).
The CK MB test provides an inside regarding the serum level of the creatine kinase-myocardial band which generally remains under 4% in normal test results. It is due to the fact that a minimal amount of the enzyme often enters the bloodstream from the salty tissues. In conditions where the CK-MB level exceeds more than 4% of the total CK in serum, it indicates the condition of muscle damage in the heart. The test is known to lag the ability to differentiate between heart attack-associated muscle damage or another source of damage within the body (Chen et al., 2022). In such conditions, other diagnostic methods are generally used in order to identify the condition of an underlying heart attack. The normal range of the enzyme in the Serum is 0 – 3.8 ng/mL, and exceedingly more than the designated range indicates muscle damage.
The normal troponin level found in the body is 0.0 – 0.4 ng/mL but a slight increase in the level of Troponin often indicates heart muscle damage associated with myocardial infarction or heart attack. The blood troponin test helps in analyzing the troponin level within the blood as well as any indicated risk of a heart attack. In case of kidney failure, decreased glomerular filtration rate leads to elevated cardiac trouble in T level which is also identified with the help of cardiac troponin blood test.
Discussion:
A differential diagnosis often takes place when the signs and symptoms indicate more than one underlying health condition and thus demands additional examination and testing to provide an appropriate diagnosis. With the help of differential diagnosis, the test to evaluate the underlying health condition narrows down and précised health assessment is carried out (Webster et al., 2017). Focusing on the case study of the patient, the serum biochemistry as well as identified biochemical test. It has been found that a state of differential diagnosis develops due to the indicated science and symptoms. The signs and symptoms as well as the serum biochemistry of the patient indicate the chance of renal failure, as well as a heart attack as both health condition, indicates similar clinical indications. After collection of the biochemical tests, it has been found that the anion gap blood test, as well as the UEC test, was found as a differential diagnostic assessment as both the tests highlight the risk of renal failure as well as underline the threat of heart attack. A low anion gap in Serum Test indicates the state of alkalosis where the blood is considered to be less acidic than the normal range. It has been found that a low level of albumin in the blood often leads to a state of low anion gap and it serves as a major indication of underlying health conditions such as kidney disease or cardiac complications (Asahina et al., 2022). It was found from the case study that the patient sustained shortness of breath as well as chain which both indicate renal failure as well as a heart attack. After the connection of the anion test, it has been found that the patient had a low anion level in the blood which thus develops a state of differential diagnosis between heart attack and renal failure.
The UEC test includes three different assessments of electrolytes and creatinine with altogether indicate the function of the kidney or any state of renal failure. It has also been found that after the conduction of electrolyte and creatinine tests, a state of differential diagnosis developed as these three examinations often indicate the risk of acute heart failure as well as renal failure. Urea nitrogen is considered a waste product that is removed from the blood by the kidney (Peng et al., 2021). When the blood contains an increased level of urea it indicates that the kidney is not functioning appropriately and at the same time increases the risk of certain cardiovascular events which includes heart failure (Jujo et al., 2017). Also after evaluation, it has been found that abnormal level of an electrolyte such as sodium potassium or manganese in blood indicates the risk of mural health conditions which mainly includes renal disease, irregular heart rhythm as well as high blood pressure. Manganese is considered to have a major influence on cardiovascular events along with potassium and calcium it plays a necessary role in managing intracellular potassium concentration. The creatinine test is carried out using a standard blood test where the creatinine level in the blood or the serum creatinine is measured. Though it has been found that serum creatinine is considered in the case of patients with renal failure but increased creatine along with worsening of the renal condition is highly common in patients with heart failure which increases during any acute heart attack episode (Vassalotti et al., 2016). Thus based on the evidence it is necessary that further a well-calculated diagnostic test is recommended to the patient in order to evaluate the underlying cause of the health condition. Based on the above discussion it has been found that the patient is suspected to suffer from major chronic kidney disease which is associated with the occurrence of cardiac complications. Thus it will be necessary to provide the patient with an appropriate chronic kidney disorder diagnosis in order to evaluate the underlying renal condition and associated complications.
Conclusion:
After evaluating and analyzing the above evidence and the biomedical test results it has been found that the patient is suspected to suffer from venal failure which is the underlying cause of cardiac complications, abnormal serum level, and shortness of breath thus it will be necessary that the patient is provided with an appropriate diagnosis which identifies the cost and provides better treatment approach. The biochemical tests provided the patients with a state of differential diagnosis as the test indicated both the condition of renal failure as well as a heart attack.
References:
Asahina, Y., Sakaguchi, Y., Kajimoto, S., Hattori, K., Doi, Y., Oka, T., ... & Isaka, Y. (2022). Time-updated anion gap and cardiovascular events in advanced chronic kidney disease: a cohort study. Clinical Kidney Journal, 15(5), 929-936. https://doi.org/10.1093/ckj/sfab277
Bamanikar, S. A., Bamanikar, A. A., & Arora, A. (2016). Study of Serum urea and Creatinine in Diabetic and nondiabetic patients in a tertiary teaching hospital. The Journal of Medical Research, 2(1), 12-15. Retrieved from: https://www.medicinearticle.com/JMR_201621_04.pdf
Chen, M., Wang, Y., Zhao, X., Zhang, J., Peng, Y., Bai, J., ... & Gao, Z. (2022). Target-responsive DNA hydrogel with microfluidic chip smart readout for quantitative point-of-care testing of creatine kinase MB. Talanta, 243, 123338. Retrieved from: https://doi.org/10.1016/j.talanta.2022.123338
Delanaye, P., Cavalier, E., & Pottel, H. (2017). Serum creatinine: not so simple!. Nephron, 136(4), 302-308. https://doi.org/10.1159/000469669
Dhanani, J. A., Barnett, A. G., Lipman, J., & Reade, M. C. (2018). Strategies to reduce inappropriate laboratory blood test orders in intensive care are effective and safe: a before-and-after quality improvement study. Anaesthesia and intensive care, 46(3), 313-320. Retrieved from: https://journals.sagepub.com/doi/pdf/10.1177/0310057X1804600309
Jujo, K., Minami, Y., Haruki, S., Matsue, Y., Shimazaki, K., Kadowaki, H., ... & Hagiwara, N. (2017). Persistent high blood urea nitrogen level is associated with increased risk of cardiovascular events in patients with acute heart failure. ESC heart failure, 4(4), 545-553. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5695177/pdf/EHF2-4-545.pdf
Kim, J., & Hashim, I. A. (2016). The clinical utility of CK-MB measurement in patients suspected of acute coronary syndrome. Clinica Chimica Acta, 456, 89-92. https://doi.org/10.1016/j.cca.2016.02.030
Lab Industries (2016), Ichroma CK-MB. Retrieved on 13 April, 2023 from: http://www.labindustrias.com/web/wp-content/uploads/2018/05/INS-CK-EN-CK-MB_Rev.07_161216-1.pdf#:~:text=ichroma%E2%84%A2%20CK%2DMB%20is,acute%20coronary%20syndrome%20%28ACS%29
Laville, S. M., Couturier, A., Lambert, O., Metzger, M., Mansencal, N., Jacquelinet, C., ... & Massy, Z. A. (2023). Urea levels and cardiovascular disease in patients with chronic kidney disease. Nephrology Dialysis Transplantation, 38(1), 184-192. Retrieved from: https://doi.org/10.1093/ndt/gfac045
Mair, J., Lindahl, B., Hammarsten, O., Müller, C., Giannitsis, E., Huber, K., ... & Jaffe, A. S. (2018). How is cardiac troponin released from injured myocardium?. European heart journal: acute cardiovascular care, 7(6), 553-560. https://doi.org/10.1177/2048872617748553
Peng, R., Liu, K., Li, W., Yuan, Y., Niu, R., Zhou, L., ... & Wu, T. (2021). Blood urea nitrogen, blood urea nitrogen to creatinine ratio and incident stroke: the Dongfeng-Tongji cohort. Atherosclerosis, 333, 1-8. https://doi.org/10.1016/j.atherosclerosis.2021.08.011
Vassalotti, J. A., Centor, R., Turner, B. J., Greer, R. C., Choi, M., Sequist, T. D., & National Kidney Foundation Kidney Disease Outcomes Quality Initiative. (2016). Practical approach to detection and management of chronic kidney disease for the primary care clinician. The American journal of medicine, 129(2), 153-162. https://doi.org/10.1016/j.amjmed.2015.08.025
Webster, A. C., Nagler, E. V., Morton, R. L., & Masson, P. (2017). Chronic kidney disease. The lancet, 389(10075), 1238-1252. https://doi.org/10.1016/S0140-6736(16)32064-5
Yang, S. W., Zhou, Y. J., Zhao, Y. X., Liu, Y. Y., Tian, X. F., Wang, Z. J., ... & Hu, D. Y. (2017). The serum anion gap is associated with disease severity and all-cause mortality in coronary artery disease. Journal of geriatric cardiology: JGC, 14(6), 392. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5540871/pdf/jgc-14-06-392.pdf
NURBN2024 Mental Health Recovery Plan Case Study Sample
Scenario: Mental Health Recovery Plan
Note: This is information is a continuation of Bens story from Task 1, all previous information and video still applies Ben, a 25-year-old qualified builder, was brought into the Emergency Department by the Police three days ago following an aggressive episode involving his girlfriend outside their house. Ben behaviour raised concerns, leading the Police to believe that he was mentally unwell and posed a risk to himself and/or others. As a result, Ben was detained and taken to the local health service. Ben has a history of depression and borderline personality disorder, with known suicide attempts. His depression has been ongoing since he was 21 years old. Additionally, he has been using substances since the age of 14. His girlfriend informed the police that his substance use had become much worse & in recent months and that he had started acting strangely Upon admission to the Emergency Department, Ben was found to have a mixture of alcohol, ice (methamphetamine), and cannabis in his system. He was also experiencing a psychotic episode. The healthcare professionals managed his acute symptoms and determined that he is now stable enough to be discharged from the inpatient unit to a community setting. However, given his complex history and current mental state, a comprehensive recovery plan is necessary to support his transition and rehabilitation. Your previous MSE and risk assessment contributed to his care and after 4 days, he is to be discharged in the community.
You have just started in the community and have requested to continue working with Ben at the Community Mental Health Service. Ben has agreed to this as he is comfortable with you, having previously met you in the Inpatient Unit. He has also been taken off the mental health act and is now a voluntary patient Ben’s Current presentation and information: Ben’s symptoms of psychosis seem to be resolved currently prescribed Olanzapine 10mg BD is also prescribed Diazepam 5mg TDS. These medications were also used as part of Ben’s withdrawal from his methamphetamine and cannabis whilst he was in hospital. Ben previously was on Diazepam 10mg TDS. The psychiatrist would like this to be reduced and will review these medications with a view to discontinuing when appropriate.
When in hospital, Ben also started a SSRI called Escitalopram 10mg Daily. The psychiatrist would like this to be monitored [AC1] with an increase to 20 mg if tolerated, Ben was [AC2] previously on other antidepressants before admission and stated, “they did nothing for him”. He has not had Escitalopram before.
Ben still presents as low in mood; he still states his girlfriend will leave him and will lose his job and is embarrassed about how he was brought into hospital. These statements appear to be related to his mood and do not fit delusional content. He has stated that he has no plans to take own his life, but he does on occasion think about if he could just go to sleep and not wakeup as his thoughts “don’t stop” sometimes and he just wants to get away.
Overall, Ben still has till has some mild symptoms of withdrawal, and this has generally been managed well in hospital with an Amphetamine Withdrawal Scale and his regular medication. He currently feels he cannot miss any doses of the Olanzapine and Diazepam, otherwise he may will “lose it”. Ben has discharged, back to his home with his girlfriend. She has been very supportive during his inpatient stay. His girlfriend is worried about future relapse. His mother Cathy has also been supportive to Ben during this time and has volunteered to help where she can. Ben’s workplace has organised him some sick leave. Ben’s girlfriend has discussed with you that his boss is very supportive around mental health issues and wants him back at work when he is ready.
INSTRUCTIONS:
Instructions for Students
Task is focused on creating a recovery plan for Ben mental health, considering his transition from inpatient care to a community setting. This assignment will help you demonstrate your understanding of recovery planning, mental health interventions, monitoring and collaboration. Please carefully read and follow the instructions provided below.
Task Overview: You are required to create a recovery plan for Ben, a 25-year-old individual who was discharged from an inpatient unit to a community setting after a recent aggressive episode and psychotic episode. Your recovery plan should address mental health history, substance use, and recovery goals, considering evidence- based interventions and a include collaborative approach involving Ben, healthcare providers, family, and support network. Recovery plan can follow structured headings of Recovery plan template (provided in assessment resources) Rubric and Scoring: Your submission will be evaluated based on the rubric provided. Each criterion carries a specific point value, and your total score will be calculated out of 60 points and weighted to 50% of total grade.
Solution
Introduction
Ben is dealing with bipolar disorder and he has history of engaging in self-harming behaviour. After improvement in his condition of psychosis, he has been transferred to community care setting. For Assignment Help, this study includes a detailed interpretation of mental health recovery plan to be considered for Ben. Detailed analysis of recovery objectives, intervention risk assessment, and relapse prevention plan has been given here.
Mental health
Recovery goals
As per MSE, Ben has poor personal hygiene and he has anxiety and stress-related issues. He is dealing with emotional instability and issues while communicating about problems faced currently thus goal for Ben is to consider current distress associated with symptoms of substance withdrawal and overthinking are mentioned below.
- To improve emotional resilience and limit anxiety within 6 months through emotional wellbeing activities to ensure a positive mindset.
- Reducing habit of overthinking and managing outbursts of emotion within 6 months for managing family, occupational personal lifestyle through improving emotional resilience.
Nursing interventions
Emotional resilience-enhancing activities during treatment of mental health disorders provide scope to improve positive emotions and ensure a sense of self-satisfaction (Prakash et al., 2020). Similarly, in context of Ben, focus needs to be placed on improving emotional resilience. Under community care setting a personal wellbeing project is applicable for Ben as it helps to limit symptoms of anxiety and stress by improving resilience. Mental wellbeing training is associated with idea of ensuring positive mental health indications such as well-being and resilience in case of depressive symptoms associated with interpersonal reasons and other causes (Riepenhausen et al., 2022). Key resources to be considered in case of well-being training include community setting and social support. In this context, resilience skills are developed through cognitive behavioural therapy (CBT). Benefits of CBT include better adaptability to adverse situations, positive coping skills, and self-regulation as well as better socialisation ability (Polizzi & Lynn, 2021). In context of case of Ben, application of CBT under wellbeing training can provide opportunities to improve positive thought processes and avoid situations of poor anger management and better self-regulation. Through application of CBT there is also possibility of avoiding issues of poor personal hygiene maintenance and better socialisation can also help improve issues in communication and language. Here community health service provider has the role of assisting Ben to improve self-awareness regarding recovery and deterioration symptoms for self-monitoring. Ben needs to be assisted with using mood chart and other self-monitoring techniques.
Family relationship and occupation
Recovery goals
Based on an assessment of mental health condition and current progress made it can be identified that Ben is dealing with issues to communicate emotions and issues with others and he has manager management issues. Currently Ben is on leave from his workplace as his employer arranged leave for his mental condition and treatment. Poor emotional management and poor hygiene management can impact family and professional life in terms of poor living arrangements and finance management. Due to poor communication and mention management Ben deals with poor relationships with family members such as his mother and girlfriend. Thus based on current situation Ben's goals for improvement are mentioned below.
- Improving positive relationships with family members and colleagues in workplace through enhancing socialisation ability within 6 months.
- Improving living arrangements and personal hygiene through enhancing self-management ability within 7 months.
Nursing interventions
Ben works as a qualified builder and due to substance misuse issues; he becomes unable to manage mention which can significantly impact his professional life. Due to a poor professional lifestyle, there can be poor financial management issues and employment opportunities can become limited. In this context, area to focus on is socialisation for better family relationships and emotional and self-management for better professional life. In this context, mild exercise such as swimming yoga, or meditation can be beneficial. Further engagement with community activities can help to improve socialisation. Meditation is beneficial for dealing with anger management issues in terms of enhancing sense of peace and calm as well as limiting anxiety and agitation due to depressive thoughts (Malakoutikhah et al., 2022). In this context supporting Ben to engage in mediation and other emotional wellbeing activities can help to improve his concentration and anger management ability to avoid negative impact of poor mention management of occupation and family life. Engaging in community activities and socialisation provide scope to avoid long-term mental health issues including Alzheimer's (Morton et al., 2021). As Ben already has a history of substance misuse and depression as well as suicide long-term effects of such conditions cannot be avoided. In this concrete, ensuring socialisation through engaging with community-based activities provides scope to retain emotional wellbeing. Thus guiding Ben to engage in socialisation activities and emotional resilience-enhancing activities as well as monitoring improvement can provide long-term outcomes.
Physical health and medication management
Recovery goals
Ben is currently under medication of Escitalopram 10 mg daily and he has a fear of developing old symptoms thus he thinks that he cannot avoid any dosage of Olanzapine and Diazepam. He is dealing with fear of engaging with substances again as he often overthinks and hallucinates about the situations. Considering physical health, poor personal hygiene is a major concern, and signs of withdrawal which include excessive thrust and weakness. Thus along with medication management, there is a need to focus on limiting signs of withdrawal and a healthy diet as there are also side effects of psychotic drugs. Considering area of physical health and medication management below-mentioned goals are applicable.
- To increase confidence and limit anxiety along with improving personal hygiene within 6 months through counselling and guided assistance.
- Engaging with family-centred activities for limiting anxiety and poor medication management along with following a healthy diet during time of withdrawal.
Nursing interventions
Ben has a history of substance abuse due to withdrawal signs his physical health can be impacted. Thus family centred interventions are beneficial for him. Involvement of family and communication about issues with family help to limit potential recurrence of substance misuse. Smiley in case of Ben communication with family members, specifically his mother, needs to be improved. Thus under supervision of community health service family-centred activities and changes in moods and wellbeing of Ben can be monitored. As he is currently under withdrawal and psychotic medication monitoring of vitals along with symptoms of withdrawal is needed. Ensuring a proper and healthy diet along with mild exercise can help to poop with symptoms of withdrawal. CBT can help Ben to overcome withdrawal stage and return to his old lifestyle. Thus as a community services provider has role to support Ben to access necessary resources and facilities.
Substance abuse
Recovery goals
Ben has overcome habit of substance misuse however signs of symptoms play a significant role in recurrence of habit. Thus signs of withdrawals need to be managed along with popper lifestyle management. Thus ensuring a scheduled lifestyle with mild exercise and socialisation can help Ben to overcome challenges of relapse. Ben has mentioned that he has no intention to harm himself but he is disturbed due to contour thoughts which cannot control. Thus to ensure concentration and lesser anxiety mindfulness training is beneficial in this case. Thus goals for substance misuse are mentioned below.
- Improving emotional resilience through mindfulness training and enhancing daily lifestyle routine of Ben within 6 months.
- Enhancing awareness regarding substance misuse and long-term effects within 2 months.
Nursing interventions
Ben is currently under signs of withdrawal and in this stage, lack of mindfulness can result in a relapse of previous situation. In this context supporting mindfulness activities and patient education regarding long-term and negative impacts of engaging with substances on health can be beneficial. In this context, a collaborative approach by engaging Ben's mother and girlfriend in a discussion regarding substance misuse and ways to consider better lifestyle management can be beneficial. Mindfulness training activities can help to ensure better self-control and enhance adaptability along with improving emotional intelligence and mental clarity (Drigas & Mitsea, 2020). In this context assisting in engaging with mindfulness training in activities can enhance Ben's self-control and ability to adapt to a new and healthy lifestyle pattern. Assisting Ben and his family to understand measures to consider for avoiding substance misuse in case of any type of psychological distress can help to ensure long-term possibility of limiting consumption of substances. Thus a family-centric approach and continuous monitoring of emotional resilience associated with mindfulness training is needed here.
Risk assessment
Ben is needed to be monitored in terms of his behaviour with family members, friends such as his girlfriend, and in his occupational life. Through proper counselling and continuous assessment of behaviour and lifestyle management activities, risk assessment can be done. A timely assessment of lifestyle behaviour and emotional resilience can provide scope to assess risk associated with potentiality of developing bipolar disorders and other psychological issues (Singh et al., 2022). In this context of behavioural assessment, there is the possibility of understanding current mental state and by interpreting interrelationship between family members and occupational performance there is possibility of determining effects of ongoing medication and treatment practises. Similarly in case of Ben through monitoring and assistance of his family members, there is possibility of determining potentiality of any risky behaviour and taking strict action in case of any potentiality of self-harming or anger management issues.
Discharge planning
During discharge, there are certain areas to be considered for avoiding mismanagement of medication, and relapse of situation including patient education and detailed assessment (Gledhill et al., 2023). In this case, while discharging Ben a patient education session follow-up check-up schedule as well as a diet plan and other physical activity and mindfulness training plan needed to be provided. Benefits of patient education during discharge include health empowerment, better health outcomes, and ensuring a better quality of life for patients (Ådnanes et al., 2020). It also reduces rate of readmission and in case of Ben due to symptoms of withdrawal through proper patient education and awareness along with collaboration of family members and his girlfriend; there is a possibility of avoiding situation of relapse. In case of Ben communicating with family members, arranging patient education sessions is beneficial. During discharge, proper details regarding physical exercises and ongoing medication along with therapies to be considered for him need to be communicated properly with family members to ensure collaboration and family centred treatment plan. In case of occupational lifestyle stress factors to be avoided in occupation also need to be communicated with Ben and his family members to reduce recurrence of substance misuse and psychotic condition.
Relapse prevention plan
Developing a relapse prevention plan requires recognising stages of relapse which are mainly three stages emotional, mental, and physical (Ociskova et al., 2022). It also becomes necessary to understand factors resulting from psychological turbulence to cause relapse of any type of psychotic symptoms. In context of Ben, there is a possibility of relapse of substance misuse habit and development of bipolar disorder along with anxiety and stress. In this context, major focus is to monitor triggers which are anxiety and depression as well as losing control over maintaining emotion. In case of any changes in behaviour such as lack of control over emotion and emotional distress, there is a need for further appointments with a psychiatrist and assistance of a community service provider to limit relapse of situation. In this context collaboration and monitoring through family members and friends is necessary as well as continuous socialisation and maintaining a lifestyle with a healthy diet and exercise can be beneficial to avoid relapse of such a situation.
Conclusion
Based on overall analysis it can be identified that in case of Ben, there is need to focus on applying CBT, physical exercises, and mindfulness training to enhance concentration and self-confidence. Engaging in mindfulness activities can help to overcome challenges of poor lifestyle and poor occupational performance. Patient and family-centric approach is considered for discharge planning and relapse prevention step-by-step monitoring of triggers is recommended.
References
.png)

- Assignment - Child Care
- Assignment - Mathematics
- Assignment - Accounting
- Assignment - Auditing
- Assignment - Biology
- Assignment - Law
- Assignment - Management
- Assignment - Nursing
- Assignment - Finance
- Assignment - Computer Science and IT
- Assignment - Humanities
- Assignment - Economics
- Assignment - Statistics
- Assignment - Architecture
- Assignment - Engineering
- Assignment - cookery
- Assignment - Marketing
- Case Study - Chemistry
- Case Study - Accounting
- Case Study - Law
- Case Study - Management
- Case Study - Nursing
- Case Study - Finance
- Case Study - Computer Science and IT
- Case Study - Engineering
- Case Study - Economics
- Case Study - Biology
- Case Study - Auditing
- Case Study - Marketing
- Case Study - Project Management
- Coursework - Diploma
- Coursework - Accounting
- Coursework - Auditing
- Coursework - Biology
- Coursework - Management
- Coursework - Nursing
- Coursework - Finance
- Coursework - Computer Science and IT
- Coursework - Engineering
- Coursework - Humanities
- Coursework - Child Care
- Coursework - Project Management
- Coursework - Economics
- Coursework - Cookery
- Coursework - Law
- Dissertation - Accounting
- Dissertation - Auditing
- Dissertation - Biology
- Dissertation - Law
- Dissertation - Management
- Dissertation - Nursing
- Dissertation - Finance
- Dissertation - Computer Science and IT
- Dissertation - Humanities
- Dissertation - Economics
- Essay - Politics
- Essay - Childcare
- Essay - Accounting
- Essay - Biology
- Essay - Law
- Essay - Management
- Essay - Nursing
- Essay - Computer Science and IT
- Essay - Humanities
- Essay - Economics
- Essay - Auditing
- Essay - Engineering
- Essay - Architecture
- Essay - Finance
- Essay - Science
- Essay - Marketing
- Programming - Computer Science and IT
- Reports - Management
- Reports - Computer Science and IT
- Reports - Project Management
- Reports - Marketing
- Reports - Nursing
- Reports - Engineering
- Reports - Accounting
- Reports - Humanities
- Reports - Finance
- Reports - Architecture
- Reports - Biology
- Reports - Economics
- Reports - Childcare
- Reports - Law
- Research - Accounting
- Research - Auditing
- Research - Biology
- Research - Law
- Research - Management
- Research - Nursing
- Research - Finance
- Research - Computer Science and IT
- Research - Science
- Research - Engineering
- Research - Humanities
- Research - Economics
- Research - Project Management
- Research - Statistics
- Research - Architecture
- Research - Marketing
- Thesis Writing - Computer Science and IT
- Thesis Writing - Engineering
- Thesis Writing - Biology
- Thesis Writing - Finance
- Thesis Writing - Humanities
- Thesis Writing - Auditing
- Thesis Writing - Economics
- Thesis Writing - Law
- Thesis Writing - Nursing
- Thesis Writing - Accounting
- Thesis Writing - Architecture

.png)
~5.png)
.png)
~1.png)



















































.png)






