Order Now
- Home
- About Us
-
Services
-
Assignment Writing
-
Academic Writing Services
- HND Assignment Help
- SPSS Assignment Help
- College Assignment Help
- Writing Assignment for University
- Urgent Assignment Help
- Architecture Assignment Help
- Total Assignment Help
- All Assignment Help
- My Assignment Help
- Student Assignment Help
- Instant Assignment Help
- Cheap Assignment Help
- Global Assignment Help
- Write My Assignment
- Do My Assignment
- Solve My Assignment
- Make My Assignment
- Pay for Assignment Help
-
Management
- Management Assignment Help
- Business Management Assignment Help
- Financial Management Assignment Help
- Project Management Assignment Help
- Supply Chain Management Assignment Help
- Operations Management Assignment Help
- Risk Management Assignment Help
- Strategic Management Assignment Help
- Logistics Management Assignment Help
- Global Business Strategy Assignment Help
- Consumer Behavior Assignment Help
- MBA Assignment Help
- Portfolio Management Assignment Help
- Change Management Assignment Help
- Hospitality Management Assignment Help
- Healthcare Management Assignment Help
- Investment Management Assignment Help
- Market Analysis Assignment Help
- Corporate Strategy Assignment Help
- Conflict Management Assignment Help
- Marketing Management Assignment Help
- Strategic Marketing Assignment Help
- CRM Assignment Help
- Marketing Research Assignment Help
- Human Resource Assignment Help
- Business Assignment Help
- Business Development Assignment Help
- Business Statistics Assignment Help
- Business Ethics Assignment Help
- 4p of Marketing Assignment Help
- Pricing Strategy Assignment Help
- Nursing
-
Finance
- Finance Assignment Help
- Do My Finance Assignment For Me
- Financial Accounting Assignment Help
- Behavioral Finance Assignment Help
- Finance Planning Assignment Help
- Personal Finance Assignment Help
- Financial Services Assignment Help
- Forex Assignment Help
- Financial Statement Analysis Assignment Help
- Capital Budgeting Assignment Help
- Financial Reporting Assignment Help
- International Finance Assignment Help
- Business Finance Assignment Help
- Corporate Finance Assignment Help
-
Accounting
- Accounting Assignment Help
- Managerial Accounting Assignment Help
- Taxation Accounting Assignment Help
- Perdisco Assignment Help
- Solve My Accounting Paper
- Business Accounting Assignment Help
- Cost Accounting Assignment Help
- Taxation Assignment Help
- Activity Based Accounting Assignment Help
- Tax Accounting Assignment Help
- Financial Accounting Theory Assignment Help
-
Computer Science and IT
- Operating System Assignment Help
- Data mining Assignment Help
- Robotics Assignment Help
- Computer Network Assignment Help
- Database Assignment Help
- IT Management Assignment Help
- Network Topology Assignment Help
- Data Structure Assignment Help
- Business Intelligence Assignment Help
- Data Flow Diagram Assignment Help
- UML Diagram Assignment Help
- R Studio Assignment Help
-
Law
- Law Assignment Help
- Business Law Assignment Help
- Contract Law Assignment Help
- Tort Law Assignment Help
- Social Media Law Assignment Help
- Criminal Law Assignment Help
- Employment Law Assignment Help
- Taxation Law Assignment Help
- Commercial Law Assignment Help
- Constitutional Law Assignment Help
- Corporate Governance Law Assignment Help
- Environmental Law Assignment Help
- Criminology Assignment Help
- Company Law Assignment Help
- Human Rights Law Assignment Help
- Evidence Law Assignment Help
- Administrative Law Assignment Help
- Enterprise Law Assignment Help
- Migration Law Assignment Help
- Communication Law Assignment Help
- Law and Ethics Assignment Help
- Consumer Law Assignment Help
- Science
- Biology
- Engineering
-
Humanities
- Humanities Assignment Help
- Sociology Assignment Help
- Philosophy Assignment Help
- English Assignment Help
- Geography Assignment Help
- Agroecology Assignment Help
- Psychology Assignment Help
- Social Science Assignment Help
- Public Relations Assignment Help
- Political Science Assignment Help
- Mass Communication Assignment Help
- History Assignment Help
- Cookery Assignment Help
- Auditing
- Mathematics
-
Economics
- Economics Assignment Help
- Managerial Economics Assignment Help
- Econometrics Assignment Help
- Microeconomics Assignment Help
- Business Economics Assignment Help
- Marketing Plan Assignment Help
- Demand Supply Assignment Help
- Comparative Analysis Assignment Help
- Health Economics Assignment Help
- Macroeconomics Assignment Help
- Political Economics Assignment Help
- International Economics Assignments Help
-
Academic Writing Services
-
Essay Writing
- Essay Help
- Essay Writing Help
- Essay Help Online
- Online Custom Essay Help
- Descriptive Essay Help
- Help With MBA Essays
- Essay Writing Service
- Essay Writer For Australia
- Essay Outline Help
- illustration Essay Help
- Response Essay Writing Help
- Professional Essay Writers
- Custom Essay Help
- English Essay Writing Help
- Essay Homework Help
- Literature Essay Help
- Scholarship Essay Help
- Research Essay Help
- History Essay Help
- MBA Essay Help
- Plagiarism Free Essays
- Writing Essay Papers
- Write My Essay Help
- Need Help Writing Essay
- Help Writing Scholarship Essay
- Help Writing a Narrative Essay
- Best Essay Writing Service Canada
-
Dissertation
- Biology Dissertation Help
- Academic Dissertation Help
- Nursing Dissertation Help
- Dissertation Help Online
- MATLAB Dissertation Help
- Doctoral Dissertation Help
- Geography Dissertation Help
- Architecture Dissertation Help
- Statistics Dissertation Help
- Sociology Dissertation Help
- English Dissertation Help
- Law Dissertation Help
- Dissertation Proofreading Services
- Cheap Dissertation Help
- Dissertation Writing Help
- Marketing Dissertation Help
- Programming
-
Case Study
- Write Case Study For Me
- Business Law Case Study Help
- Civil Law Case Study Help
- Marketing Case Study Help
- Nursing Case Study Help
- Case Study Writing Services
- History Case Study help
- Amazon Case Study Help
- Apple Case Study Help
- Case Study Assignment Help
- ZARA Case Study Assignment Help
- IKEA Case Study Assignment Help
- Zappos Case Study Assignment Help
- Tesla Case Study Assignment Help
- Flipkart Case Study Assignment Help
- Contract Law Case Study Assignments Help
- Business Ethics Case Study Assignment Help
- Nike SWOT Analysis Case Study Assignment Help
- Coursework
- Thesis Writing
- CDR
- Research
-
Assignment Writing
-
Resources
- Referencing Guidelines
-
Universities
-
Australia
- Asia Pacific International College Assignment Help
- Macquarie University Assignment Help
- Rhodes College Assignment Help
- APIC University Assignment Help
- Torrens University Assignment Help
- Kaplan University Assignment Help
- Holmes University Assignment Help
- Griffith University Assignment Help
- VIT University Assignment Help
- CQ University Assignment Help
-
Australia
- Experts
- Free Sample
- Testimonial
LMED28002 Haematopathology Case study 1 Sample
A 20 year old pregnant woman from Mumbai went to her GP complaining of lethargy, and shortness of breath. As she was pregnant she was admitted to an obstetrics hospital for investigation. Clinical symptoms showed pale conjunctiva, tachycardia and mild spooning of nails. She reported unusual dietary cravings.
The results of an initial Full Blood Count from a Sysmex XN-1000 analyser are shown below:
.png)
A Wright’s stained peripheral blood smear showed this morphology:
.png)
Further testing was requested, and the results and methods are shown below:
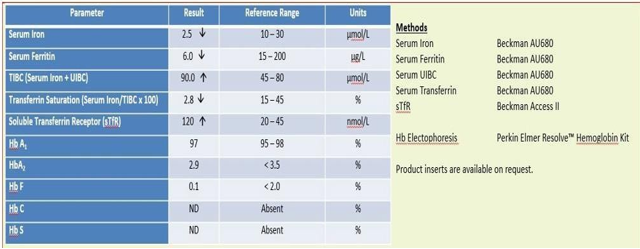
As described the following methods were used to achieve these results, details of each method are included in subsequent pages.
Full Blood Count
Blood collection was by a standard venepuncture technique of the antecubital vein with the blood collected into a Vacutainer® tube containing K2EDTA.
Analysis was completed within 30 minutes of collection, the Haemoglobin and cell counts were performed using the Sysmex XN-1000 analyser and the smear was prepared using the manual wedge technique.
Smears were stained manually using Wright’s stain.
Biochemistry
Blood collection was by a standard venepuncture technique of the antecubital vein with the blood collected into a Vacutainer® Serum Spearation Tube (SST™).
The blood was mixed by inverting the tube 5 times and allowed to stand for 30 minutes prior to centrifugation for 10 minutes at 1,200 g.
Analysis was completed within 30 minutes of centrifugation, the Iron Studies including Iron, Ferritin, Transferrin and UIBC were performed using the Beckman Coulter AU680 analyser.
The Soluble Transferrin Receptor assay was performed using the Beckman Coulter Access II analyser.
Electrophoresis
The Haemoglobin Electrophoresis was performed using the Perkin Elmer RESOLVE™ Hemoglobin Kit on the blood used for the Full Blood Count.
Solution
Abstract
A pregnant woman in her 20s from Mumbai presented with unusual dietary cravings, lethargy, and shortness of breath. She had mild nail spooning, pale conjunctiva, and tachycardia. Her full blood count revealed microcytic hypochromic red cells, low hemoglobin (60 g/L), low hematocrit (21 L/L), and an increased red cell distribution width. Studies on iron revealed low levels of iron, ferritin, and transferrin, all of which are indicative of iron deficiency anemia. Electrophoresis of hemoglobin was normal. She was treated with iron supplements and regular visits to obstetricians to monitor fetal growth. This case for the assignment help demonstrates how crucial it is for pregnant women to be diagnosed and treated for iron deficiency anemia as soon as possible.
Introduction
A 20-year-old pregnant lady from Mumbai was introduced to her GP with dormancy and windedness, prompting admission to an obstetrics emergency clinic for additional examination. The patient reported unusual dietary cravings, pale conjunctiva, tachycardia, and mild nail spooning on clinical examination (Yeoh, and Chiew, 2022). A Sysmex XN-1000 analyzer's Full Blood Count (FBC) revealed anemia with a high red cell distribution width and low hemoglobin, hematocrit, and mean cell volume. The elevated count of reticulocytes points to a possible compensatory response. White cell and platelet counts were within acceptable ranges. The Beckman Coulter AU680 analyzer was utilized for the iron investigations, which included ferritin, transferrin, and unsaturated iron-restricting limit (UIBC). The soluble transferrin receptor assay was performed with the Beckman Coulter Access II analyzer. On the blood that was used for the FBC, the Perkin Elmer RESOLVETM Hemoglobin Pack was used to perform hemoglobin electrophoresis. A clinical examination revealed anemia with a wide red cell distribution and low hemoglobin, hematocrit, and mean cell volume. The unsaturated iron-binding capacity and soluble transferrin receptor assay, as well as the iron, ferritin, and transferrin studies, were carried out. The hemoglobin electrophoresis was carried out. The number of reticulocytes was up, which could be a response to compensate. These findings point to an underlying possibility of iron deficiency anemia during pregnancy, which calls for additional investigation and appropriate treatment.
Materials and methods
Standard venipuncture was used to collect blood from the antecubital vein for the Full Blood Count and Iron Studies. The blood was collected using a Vacutainer® tube containing K2EDTA for FBC and a Vacutainer® Serum Separation Tube (SSTTM) for Iron Studies. The FBC analysis was performed with the Sysmex XN-1000 analyzer. The smear was stained manually with Wright's stain and prepared using the manual wedge method. For the Iron Studies, which included iron, ferritin, transferrin, and UIBC, a Beckman Coulter AU680 analyzer was utilized. The Soluble Transferrin Receptor assay was performed with the Beckman Coulter Access II analyzer. The Perkin Elmer RESOLVETM Hemoglobin Kit was used to conduct the hemoglobin electrophoresis on the same blood sample that was used for the Full Blood Count. All tests were analyzed within 30 minutes of collection or centrifugation.
Results
Haemoglobin (Hb) and Haemoglobin (Hb) and hematocrit (Hct) levels are significantly lower in the FBC results, indicating anemia. Both the mean cell hemoglobin concentration (MCHC) and the low mean cell volume (MCV) point to microcytic anemia. The elevated red cell distribution width (RDW) indicates that the size of red blood cells (RBCs) varies. The reticulocyte count is slightly higher, indicating that the bone marrow is producing new RBCs in response. The white blood cell count (WBC) is slightly elevated, with a predominant neutrophil population, but the platelet count is within the normal reference range.
.png)
Figure 1: Full Blood Count from a “Sysmex XN-1000” analyser
(Source: Provided)
Any abnormal variants of hemoglobin that may be present can be identified with the aid of the hemoglobin electrophoresis test. The iron studies will provide information on iron stores, transferrin saturation, and iron binding capacity in terms of biochemistry, which can assist in determining the cause of the anemia. The soluble transferrin receptor assay can also give you more information about how much iron is in your body. By and large, the FBC and resulting tests recommend a finding of iron-lack weakness. The strange dietary desires revealed by the patient may likewise uphold this analysis. The GP ought to give fitting iron supplementation and screen the patient's reaction to treatment. The obstetric group ought to likewise intently screen the patient's pregnancy and guarantee ideal consideration.
Discussion
The pregnant lady has extreme pallor, as per the FBC results. Her mean cell volume (MCV) is low at 55 fL, indicating that she has microcytic anemia, and her hemoglobin (Hb) level is 60 g/L, which is significantly lower than the reference range of 115-165 g/L. Her red cell count (RCC) is also significantly lower than the reference range, at 3.82 x 1012/L, and her hematocrit (Hct) is significantly lower, at 21 L/L (Obeid et al., 2019). Low concentrations of MCHC and mean cell hemoglobin (MCH) point to hypothermia. A high degree of anisocytosis is indicated by a 19.1% rise in the red cell distribution width (RDW). The reticulocyte count (Retics), which is within the reference range at 1.7%, indicates that the bone marrow's response to the anemia is normal. Neutrophils (N) are slightly elevated on the differential white cell count (Diff) at 4.8 x 109/L, while lymphocytes (L), monocytes (M), eosinophils (E), and basophils (B) fall within the normal range. The white cell count (WCC) and platelet count (Plts) are both within the reference range. At 569 x 109/L, the platelet count is slightly elevated.
Iron deficiency anemia, the most common cause of anemia during pregnancy, appears to be the diagnosis made by the FBC results for the pregnant woman (Samarron et al., 2020). Iron is required for the production of hemoglobin, and since maternal red cell mass and fetal requirements increase during pregnancy, iron requirements rise as well. Iron deficiency anemia is suggested by the low Hb, RCC, and Hct is values. Because this is a characteristic morphological feature of iron deficiency anemia, the high RDW of microcytic, hypochromic red cells also suggests iron deficiency. The bone marrow is effectively counteracting the anemia, as evidenced by the normal reticulocyte count.
As thrombopoietin, a hormone produced by the liver and kidney is stimulated in response to anemia, leading to an increase in platelet production, the elevated platelet count is likely the result of the compensatory response to the anemia. The normal Diff and WCC results indicate that the anemia is not caused by an underlying infection or inflammation.
Serum iron, ferritin, transferrin, and unsaturated iron-binding capacity (UIBC) studies would be the next step in the investigation of this woman's anemia (Wu et al., 2021). The results of these tests will assist in confirming the diagnosis of iron deficiency anemia and determining its severity. Additionally, the soluble transferrin receptor assay (sTfR) can be used to distinguish between microcytic anemia caused by other conditions like thalassemia and iron deficiency anemia.
The clinical signs of sluggishness, shortness of breath, and unusual food cravings support the diagnosis of iron deficiency anemia (Hall, 2020). Fatigue, weakness, shortness of breath, and pica—a craving for things other than food like ice or dirt—are all symptoms of iron deficiency.
Inadequate iron intake from food is the most common cause of iron deficiency anemia, but it can also be caused by excessive blood loss or poor iron absorption in the gastrointestinal tract. In this instance, the patient said that she had unusual food cravings, which could mean that she didn't have enough iron or other nutrients. Additionally, her shortness of breath and lethargy are indicative of anemia. The full blood count reveals a significant drop in hemoglobin, hematocrit, and mean cell volume, all of which point to a smaller red blood cell mass. Hypochromia is indicated by a decrease in the mean cell hemoglobin concentration. A high red cell distribution width and these findings suggest that the anemia is microcytic and likely caused by iron deficiency (Carville, 2021). The reticulocyte count is marginally raised, showing a reaction to pallor, and the platelet count is raised, which can be a compensatory system for diminished oxygen conveyance to tissues. The fact that the differential and white cell count are within normal ranges suggests that the anemia is not caused by an infection or a hematologic malignancy. Hemoglobin electrophoresis and iron studies can be used to confirm the diagnosis and identify the underlying cause of the anemia.
In conclusion, the findings of the FBC suggest that the Mumbai-based pregnant woman, who is 20 years old, suffers from severe iron deficiency anemia. The most common cause of anemia during pregnancy is iron deficiency, which can have significant negative effects on both the mother and the fetus. Iron tests would be the next step in the investigation to confirm the diagnosis and determine the severity of the iron deficiency. Corrective treatment requires iron supplementation.
References
.png)

Download Samples PDF
Related Sample
- GDECE101 Early Childhood Care and Education
- 7138SOH Global Healthcare Challenges Assignment
- BST720 Leadership Work and Organization Assignment
- MBA504 Data Analytics for Business Assignment
- MANU1381 Sustainable Engineering Systems and Environment Assignment
- MBA643 Project Initiation Planning and Execution
- SITXINV001 Receive and Store Stock Assignment
- BUACC5930 Accounting Concepts and Practice Essay
- MBA642 Project Initiation, Planning and Execution Assignment
- BUECO5903 Business Economics Assignment Part A
- ITBO201 IT for Business Organisations Assignment
- Business Capstone Project Assignments
- NURS3015 Health Variations 4 Assignment
- MBA632 Knowledge Management Assignment
- ITECH7407 Real Time Analytics Assignment
- PROJ6003 Project Execution and Control
- FNCE623 Capital Budgeting Assignment Report 1
- ITSU2011 Computational Mathematics Assignment
- CVE80010 Principles of Sustainability Assignment
- DATA4700 Digital Marketing and Competitive Advantage Report 3
Assignment Services
-
Assignment Writing
-
Academic Writing Services
- HND Assignment Help
- SPSS Assignment Help
- College Assignment Help
- Writing Assignment for University
- Urgent Assignment Help
- Architecture Assignment Help
- Total Assignment Help
- All Assignment Help
- My Assignment Help
- Student Assignment Help
- Instant Assignment Help
- Cheap Assignment Help
- Global Assignment Help
- Write My Assignment
- Do My Assignment
- Solve My Assignment
- Make My Assignment
- Pay for Assignment Help
-
Management
- Management Assignment Help
- Business Management Assignment Help
- Financial Management Assignment Help
- Project Management Assignment Help
- Supply Chain Management Assignment Help
- Operations Management Assignment Help
- Risk Management Assignment Help
- Strategic Management Assignment Help
- Logistics Management Assignment Help
- Global Business Strategy Assignment Help
- Consumer Behavior Assignment Help
- MBA Assignment Help
- Portfolio Management Assignment Help
- Change Management Assignment Help
- Hospitality Management Assignment Help
- Healthcare Management Assignment Help
- Investment Management Assignment Help
- Market Analysis Assignment Help
- Corporate Strategy Assignment Help
- Conflict Management Assignment Help
- Marketing Management Assignment Help
- Strategic Marketing Assignment Help
- CRM Assignment Help
- Marketing Research Assignment Help
- Human Resource Assignment Help
- Business Assignment Help
- Business Development Assignment Help
- Business Statistics Assignment Help
- Business Ethics Assignment Help
- 4p of Marketing Assignment Help
- Pricing Strategy Assignment Help
- Nursing
-
Finance
- Finance Assignment Help
- Do My Finance Assignment For Me
- Financial Accounting Assignment Help
- Behavioral Finance Assignment Help
- Finance Planning Assignment Help
- Personal Finance Assignment Help
- Financial Services Assignment Help
- Forex Assignment Help
- Financial Statement Analysis Assignment Help
- Capital Budgeting Assignment Help
- Financial Reporting Assignment Help
- International Finance Assignment Help
- Business Finance Assignment Help
- Corporate Finance Assignment Help
-
Accounting
- Accounting Assignment Help
- Managerial Accounting Assignment Help
- Taxation Accounting Assignment Help
- Perdisco Assignment Help
- Solve My Accounting Paper
- Business Accounting Assignment Help
- Cost Accounting Assignment Help
- Taxation Assignment Help
- Activity Based Accounting Assignment Help
- Tax Accounting Assignment Help
- Financial Accounting Theory Assignment Help
-
Computer Science and IT
- Operating System Assignment Help
- Data mining Assignment Help
- Robotics Assignment Help
- Computer Network Assignment Help
- Database Assignment Help
- IT Management Assignment Help
- Network Topology Assignment Help
- Data Structure Assignment Help
- Business Intelligence Assignment Help
- Data Flow Diagram Assignment Help
- UML Diagram Assignment Help
- R Studio Assignment Help
-
Law
- Law Assignment Help
- Business Law Assignment Help
- Contract Law Assignment Help
- Tort Law Assignment Help
- Social Media Law Assignment Help
- Criminal Law Assignment Help
- Employment Law Assignment Help
- Taxation Law Assignment Help
- Commercial Law Assignment Help
- Constitutional Law Assignment Help
- Corporate Governance Law Assignment Help
- Environmental Law Assignment Help
- Criminology Assignment Help
- Company Law Assignment Help
- Human Rights Law Assignment Help
- Evidence Law Assignment Help
- Administrative Law Assignment Help
- Enterprise Law Assignment Help
- Migration Law Assignment Help
- Communication Law Assignment Help
- Law and Ethics Assignment Help
- Consumer Law Assignment Help
- Science
- Biology
- Engineering
-
Humanities
- Humanities Assignment Help
- Sociology Assignment Help
- Philosophy Assignment Help
- English Assignment Help
- Geography Assignment Help
- Agroecology Assignment Help
- Psychology Assignment Help
- Social Science Assignment Help
- Public Relations Assignment Help
- Political Science Assignment Help
- Mass Communication Assignment Help
- History Assignment Help
- Cookery Assignment Help
- Auditing
- Mathematics
-
Economics
- Economics Assignment Help
- Managerial Economics Assignment Help
- Econometrics Assignment Help
- Microeconomics Assignment Help
- Business Economics Assignment Help
- Marketing Plan Assignment Help
- Demand Supply Assignment Help
- Comparative Analysis Assignment Help
- Health Economics Assignment Help
- Macroeconomics Assignment Help
- Political Economics Assignment Help
- International Economics Assignments Help
-
Academic Writing Services
-
Essay Writing
- Essay Help
- Essay Writing Help
- Essay Help Online
- Online Custom Essay Help
- Descriptive Essay Help
- Help With MBA Essays
- Essay Writing Service
- Essay Writer For Australia
- Essay Outline Help
- illustration Essay Help
- Response Essay Writing Help
- Professional Essay Writers
- Custom Essay Help
- English Essay Writing Help
- Essay Homework Help
- Literature Essay Help
- Scholarship Essay Help
- Research Essay Help
- History Essay Help
- MBA Essay Help
- Plagiarism Free Essays
- Writing Essay Papers
- Write My Essay Help
- Need Help Writing Essay
- Help Writing Scholarship Essay
- Help Writing a Narrative Essay
- Best Essay Writing Service Canada
-
Dissertation
- Biology Dissertation Help
- Academic Dissertation Help
- Nursing Dissertation Help
- Dissertation Help Online
- MATLAB Dissertation Help
- Doctoral Dissertation Help
- Geography Dissertation Help
- Architecture Dissertation Help
- Statistics Dissertation Help
- Sociology Dissertation Help
- English Dissertation Help
- Law Dissertation Help
- Dissertation Proofreading Services
- Cheap Dissertation Help
- Dissertation Writing Help
- Marketing Dissertation Help
- Programming
-
Case Study
- Write Case Study For Me
- Business Law Case Study Help
- Civil Law Case Study Help
- Marketing Case Study Help
- Nursing Case Study Help
- Case Study Writing Services
- History Case Study help
- Amazon Case Study Help
- Apple Case Study Help
- Case Study Assignment Help
- ZARA Case Study Assignment Help
- IKEA Case Study Assignment Help
- Zappos Case Study Assignment Help
- Tesla Case Study Assignment Help
- Flipkart Case Study Assignment Help
- Contract Law Case Study Assignments Help
- Business Ethics Case Study Assignment Help
- Nike SWOT Analysis Case Study Assignment Help
- Coursework
- Thesis Writing
- CDR
- Research

.png)
~5.png)
.png)
~1.png)



















































.png)






